It’s that time again for another helping of the naked tales of a studying physio. So let’s pick up from where we left off. If you want a refresh of part 1 you can do so here
Treatment History
The patient’s spinal fractures were managed conservatively over the course of 5 months with a spinal brace and neck brace, and through a brief period of physiotherapy at a City Hospital. Throughout the 5-month period of wearing the back brace he continued to complain of pain in his mid back, which was managed with Tramadol 50mg once or twice a day, and non steroidal anti-Inflammatory medication, which he had since cut down significantly due to stomach pains. Prior to this the patient resorted to extreme measures of taking frequent dosages of tramadol and anti-inflammatory medication in a desperate attempt to control his pain. Up until September 2015 the patient had received no further treatment. His case was re-opened and an assessment with a psychiatrist had resulted in an upsetting outcome. He reported that he and the psychiatrist had not communicated well, and he strongly disagreed with the diagnosis of Somatoform Disorder that had been provided at the time. This had caused him a great deal of distress, due to feeling unheard and disbelieved by others. The patient also felt that it was an “unsafe” diagnosis to make, and did not take his whole situation into account. This is consistent with the literature regarding acknowledgement and validation of individual experiences and perpetuation of pain experiences (Darlow et al., 2013; Greville-Harris & Dieppe, 2015; Nijs et al., 2013).
The patient met with an orthopaedic surgeon on 16 December 2015, and was referred for a bone scan of his spine. This scan was conducted on 21 December 2015; the report noted “Based on the degree of uptake of radiopharmaceutical, both the C6-7 region and the T10-11 region are potential sources for the current pain. The recent CT and MRI studies have shown significant degenerative changes at these levels with no other detectable pathology.” The patient had reportedly been advised that a surgical procedure (including fusion) at the T10-11 site might be useful in alleviating some of his pain symptoms (although this was not guaranteed). The patient reported that “a weight’s come off my shoulders” as a result of identifying a physical cause for his pain, and his mood had improved significantly as a result.

Current Management
The patient had received very little pain management to date except for use of strong opioid (Tramadol) medication that he had taken since his discharge from hospital. He had received no further allied health input since his discharge from hospital.
Beliefs
The patient presented with strong beliefs towards the fragility of his spine as a result of the explanation he had received for his ongoing pain and the need for a spinal fusion procedure. Beliefs have been shown to have a significant impact on pain experiences (O’Keeffe et al., 2015), and are also closely linked with disability and persistent widespread pain (Nijs et al., 2013). The patient’s most recent sets of imaging, which included an MRI scan, CT scan and bone scan in December 2015 showed 1) No obvious spinal cord damage or impingement, 2) No alkalosis of the sacral iliac joints with osteoarthritis in both hip joints, 3) Well healed T5 and T7 fractures with slightly increased thoracic kyphosis, 4) Calcification in the T10/T11 disc, and 6) Increased uptake at C6/C7 and T10/T11 regions. His orthopaedic surgeon indicated that the calcification at the T10/11 are the sources of his pain. On discussion with his orthopaedic surgeon about the pain in his back the patient understood that “Due to the disc collapse and the calcification of the disc”, there was a likelihood of it “growing into his spinal cord”. After further questioning, it was the understanding of the patient that he would be at risk of being rendered at worst “paraplegic” and at best “confined to a wheelchair” if he did not have spinal fusion surgery. The patient reported to have asked what his prognosis would be without a spinal fusion procedure. The orthopaedic specialist responded, “that it wasn’t going to get any better without surgery”. This left the patient feeling like his back was a “ticking time bomb” and that due to the instability in his back it was best to minimise movement of the spine. These inflated beliefs are indicative of catastrophisation and kinesiophobia (Thomas et al., 2010). The beliefs also coincided with overt pain behaviours (Vlaeyen & Linton, 2000). Pain behaviours are habitual that range from obvious limping, rubbing and guarding to tensing, grimacing and moaning. Furthermore, he recalled a time where he got into a conversation with another member of the public that was confined to a mobility scooter. The person using the mobility scooter reported a very similar experience of back pain resulting in his current situation. This further reaffirmed the patient’s thinking that his spine was not stable and that a spinal fusion would prevent the inevitable confinement to a wheelchair.
A pain catastrophizing scale (Sullivan, Bishop, & Pivik, 1995) was selected as it provides a measure of how patients ruminate and magnify their pain and also feelings of helplessness towards managing their pain. The patient scored a total of 16 (40th percentile) which placed the patient in the average range for catastrophizing.
The patient also reported that his father had been in a major road traffic accident and sustained injuries very similar to his. This had increased his awareness of the difficulties his father faced.
Coping Strategies
The patient reported to have gone through a week-long alcohol detox programme in 2013, and to have been abstinent ever since. He acknowledged that he had used alcohol as a painkiller between 2011 – 2013 and he continued to smoke cigarettes to try and alleviate anxiety that he experiences in relation to his pain. He is currently on antidepressant medication (Citalopram), and has recently attempted to engage in tai chi, which he reported to have regularly participated in prior to his accident.
The patient stated that in the past he had taken up to eight 50mg Tramadol tablets per day. This was out of desperation to control his pain, which is excessive and a further example of an overt pain behaviour. However, he was now generally only taking one tablet (two at the most on days when his pain was particularly bad). He stated that he was pleased at having reduced his pain medication.
He reported having received a small amount of psychological treatment, and when experiencing pain and psychological distress he would lie down flat and complete slow breathing exercises and positive affirmations. Lying down was also beneficial in taking some of the pressure off his back. He also reported that moderate walking helped alleviate his morning leg pain, although he needed to be careful not to overdo this.
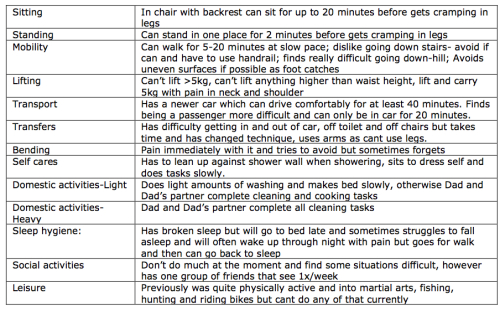
Functional Impact
Since his injury he has found ADLs increasingly difficult, particularly those that involve lifting, pulling and pushing (Figure. 3). Conversely, the patient noted that his pain had improved in the last 3 months. This is an interesting example of ongoing disability despite the improvement of pain (Ferreira et al., 2010). The Pain Disability Index was selected as it provides moderate test – retest reliability in discriminating between low and high disability in patients with persistent pain (Tait et al., 1987). The patient scored a total of 51 (83rd Percentile) indicating a high range of disability associated with his pain.
Mood, Sleep, Concentration
The patient reported having severe bouts of depression and anxiety following his injury and had issues with suicidal thoughts. Completing a Depression Anxiety Stress Scale (DASS) the results indicated that he currently displays moderate levels of depression, severe levels of stress, and extremely severe levels of anxiety. This is also consistent with the literature particularly around worry and anxiety and the perpetuation of pain states (Eccleston & Crombez, 2007).
The patient reported ongoing cognitive difficulties, particularly in the domain of memory. This can make him irritable and frustrated causing him to experience elevated levels of stress.
It was noted that the patient has intermittent disturbance of his sleep particularly when his pain is bad but generally he reports to sleep up to 7-8 hours a night.
Social Impact
The patient currently lives with his father. He returned to live with his father following the separation of his marriage prior to his accident and also due to financial distress following the injury. The patient reported that he is “a bit of a recluse” socially as he is self-conscious of being unemployed and living with his father. He is also reluctant to engage with other people as they “don’t know what it’s like to have my pain”. He stated that he was gradually trying to increase his daily activities, in particular his walking, in order to be around people. He stated that he was still prone to cognitive overload in busy environments (such as shopping centres), and also experienced a headache after more than about 10 minutes if in the sun. He reported that he had a small group of friends he saw up to twice a week; they all drank alcohol, although he was not tempted to do so.
Work Issues
The patient returned to work 9 months following the initial injury, which he feels was too early after his accident. He also reported that there was pressure from workers compensation(WC) to return to work due to the fact there was no physical cause for his ongoing pain. He continued to work and endure his pain for the next couple of years until March 2015, when he was asked to leave due to his increasing pain levels, a change in his personality and his ongoing memory issues.
He received a benefit for approximately nine months, which brought about significant financial stress. More recently, he contacted WC with the aim of reopening his file, and was eventually provided with a lump sum payment (which cleared his financial debts) and restarted on weekly compensation. Currently, weekly compensation from WC is the patient’s only form of income.
Let’s leave it there for this part as I am suitably impressed if you have managed to read this far and not drifted off to la-la land. Part 3 and the final instalment will be coming next week.
Thanks for having a read
TNP
References
Armon, C., Argoff, C. E., Samuels, J., & Backonja, M.-M. (2007). Assessment: use of epidural steroid injections to treat radicular lumbosacral pain. Neurology, 68, 723–729. http://doi.org/10.1212/01.wnl.0000256734.34238.e7
Barker, K. L., Reid, M., & Minns Lowe, C. J. (2009). Divided by a lack of common language? A qualitative study exploring the use of language by health professionals treating back pain. BMC Musculoskeletal Disorders, 10, 123. http://doi.org/10.1186/1471-2474-10-123
Barker, K. L., Reid, M., & Minns Lowe, C. J. (2014). What does the language we use about arthritis mean to people who have osteoarthritis? A qualitative study. Disability and Rehabilitation, 36(5), 367–372. http://doi.org/10.3109/09638288.2013.793409
Borg, G. A. (1982). Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise, 14(5), 377–381. http://doi.org/10.1249/00005768-198205000-00012
Chou Roger , MD; Qaseem Amir , MD, PhD, MHA; Snow Vincenza , MD; Casey Donald , MD, MPH, MBA; Cross Jr J. Thomas ., MD, MPH; Shekelle Paul , MD, PhD; and Owens Douglas K. , MD, M. (2007). Clinical Guidelines Diagnosis and Treatment of Low Back Pain : A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society, (July 2007).
Clark, B. C., Goss, D. A., Walkowski, S., Hoffman, R. L., Ross, A., & Thomas, J. S. (2011). Neurophysiologic effects of spinal manipulation in patients with chronic low back pain. BMC Musculoskeletal Disorders, 12, 170. http://doi.org/10.1186/1471-2474-12-170
Darlow, B., Dowell, A., Baxter, G. D., Perry, M., Mathieson, F., Perry, M., & Dean, S. (2013). The Enduring Impact of What Clinicians Say to People With Low Back Pain. Annals of Family Medicine, 11(6), 527–534. http://doi.org/10.1370/afm.1518.INTRODUCTION
Deyo, R. a, Mirza, S. K., Turner, J. a, & Martin, B. I. (2009). Overtreating chronic back pain: time to back off? Journal of the American Board of Family Medicine : JABFM, 22(1), 62–68. http://doi.org/10.3122/jabfm.2009.01.080102
Eccleston, C., & Crombez, G. (2007). Worry and chronic pain : A misdirected problem solving model. Pain, 132(3), 233–236. http://doi.org/10.1016/j.pain.2007.09.014
Ferreira, M. L., Machado, G., Latimer, J., Maher, C., Ferreira, P. H., & Smeets, R. J. (2010). Factors defining care-seeking in low back pain - A meta-analysis of population based surveys. European Journal of Pain, 14(7), 747.e1–747.e7. http://doi.org/10.1016/j.ejpain.2009.11.005
Greville-Harris, M., & Dieppe, P. (2015). Bad is more powerful than good: The nocebo response in medical consultations. American Journal of Medicine, 128(2), 126–129. http://doi.org/10.1016/j.amjmed.2014.08.031
Hoffmann, T., Del Mar, C., Strong, J., & Mai, J. (2013). Patients’ expectations of acute low back pain management: implications for evidence uptake. BMC Family Practice, 14(1), 7. Retrieved from http://www.biomedcentral.com/1471-2296/14/7
Hoy, D., Bain, C., Williams, G., March, L., Brooks, P., Blyth, F., … Buchbinder, R. (2012). A systematic review of the global prevalence of low back pain. Arthritis and Rheumatism, 64(6), 2028–2037. http://doi.org/10.1002/art.34347
Hoy, D., March, L., Brooks, P., Blyth, F., Woolf, A., Bain, C., … Buchbinder, R. (2014). The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Annals of the Rheumatic Diseases, 73(6), 968–974. http://doi.org/10.1136/annrheumdis-2013-204428
Kamper, S. J., Apeldoorn, A. T., Chiarotto, A., Smeets, R. J. E. M., Ostelo, R. W. J. G., Guzman, J., & van Tulder, M. W. (2015). Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ (Clinical Research Ed.), 350(February), h444. http://doi.org/10.1136/bmj.h444
Kumar, S., Beaton, K., & Hughes, T. (2013). The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews. International Journal of General Medicine, 6, 733–41. http://doi.org/10.2147/IJGM.S50243
Liddle, S. D., Baxter, G. D., & Gracey, J. H. (2007). Chronic low back pain: patients’ experiences, opinions and expectations for clinical management. Disability and Rehabilitation, 29(776008562), 1899–1909. http://doi.org/10.1080/09638280701189895
Linton, S. J. (2000). A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976), 25(9), 1148–1156. http://doi.org/10.1097/00007632-200005010-00017
McBeth, J., & Jones, K. (2007). Epidemiology of chronic musculoskeletal pain. Best Practice & Research. Clinical Rheumatology, 21(3), 403–25. http://doi.org/10.1016/j.berh.2007.03.003
Nijs, J., Roussel, N., van Wilgen, P. C., Koke, A., & Smeets, R. (2013). Thinking beyond muscles and joints: Therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Manual Therapy, 18(2), 96–102. http://doi.org/10.1016/j.math.2012.11.001
O’Keeffe, M., Purtill, H., O’Sullivan, P., Dankaerts, W., Conneely, M., Hurley, J., … O’Sullivan, K. (2015). Comparative effectiveness of active interventions for non-specific chronic spinal pain: Physical, behavioural or combined? A systematic review and meta-analysis. Physiotherapy (United Kingdom), 101, eS1131–eS1132. http://doi.org/10.1016/j.jpain.2016.01.473
Ramond, A., Bouton, C., Richard, I., Roquelaure, Y., Baufreton, C., Legrand, E., & Huez, J. F. (2011). Psychosocial risk factors for chronic low back pain in primary care-a systematic review. Family Practice. http://doi.org/10.1093/fampra/cmq072
Skelton, J. R., Wearn, A. M., & Hobbs, F. D. R. (2002). A concordance-based study of metaphoric expressions used by general practitioners and patients in consultation. British Journal of General Practice, 52(475), 114–118.
Sullivan, M. J. L., Bishop, S. R., & Pivik, J. (1995). The Pain Catastrophizing Scale: Development and validation, 7(4), 524–532. Retrieved from http://www.scopus.com/inward/record.url?eid=2-s2.0-0029584617&partnerID=40&md5=7f8615d1b52cbabde152c2e9b9683fff
Tait, C.R. Pollard, C.A. Margolis, R.B. Duckro, P.N. Krause, S. J. (1987). The Pain Disability Index: Psychometric and Validity Data. Archives of Physical Medicine and Rehabilitation.
Thomas, E. N., Pers, Y. M., Mercier, G., Cambiere, J. P., Frasson, N., Ster, F., … Blotman, F. (2010). The importance of fear, beliefs, catastrophizing and kinesiophobia in chronic low back pain rehabilitation. Annals of Physical and Rehabilitation Medicine, 53(1), 3–14. http://doi.org/10.1016/j.rehab.2009.11.002
Vertue, F. M., & Haig, B. D. (2008). An Abductive Perspective on Clinical Reasoning and Case Formulation. Journal of Clinical Psychology, 64(9), 1046–1068. http://doi.org/10.1002/jclp
Vlaeyen, J. W. S., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain, 85(3), 317–332. http://doi.org/10.1016/S0304-3959(99)00242-0
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., … Moradi-Lakeh, M. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2163–2196. http://doi.org/10.1016/S0140-6736(12)61729-2
Walsh, D. A., & Radcliffe, J. C. (2002). Pain beliefs and perceived physical disability of patients with chronic low back pain. Pain, 97(1-2), 23–31. http://doi.org/10.1016/S0304-3959(01)00426-2
Xu, N., Wei, F., Liu, X., Jiang, L., & Liu, Z. (2016). Calcific discitis with giant thoracic disc herniations in adults. European Spine Journal, 1–5. http://doi.org/10.1007/s00586-016-4402-y
Yelland, M. (2011). What do patients really want to know? International Musculoskeletal Medicine, 33(1), 1–2.

Howdy would you mind letting me know which webhost you’re working
with? I’ve loaded your blog in 3 different internet browsers and
I must say this blog loads a lot quicker then most. Can you
recommend a good web hosting provider at a reasonable price?
Thank you, I appreciate it!
LikeLike