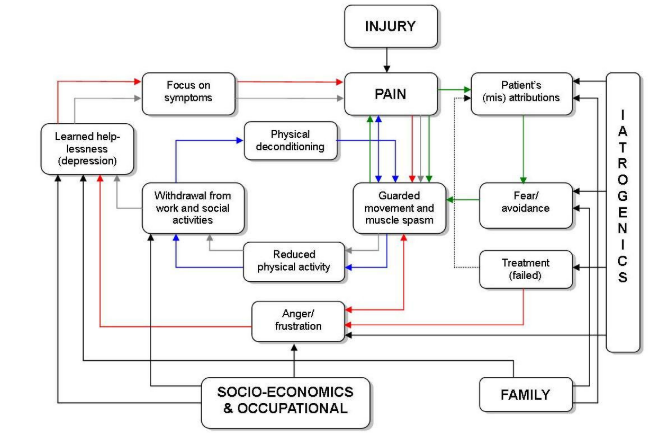
A common experience for people living with pain is the enigmatic behavior of pain. People feel a lack of control due to the unpredictability, intensity or severity of pain. This can significantly affect a person’s ability to achieve a desired outcome, such as playing with their kids, being able to vacuum, being able to work, being a supportive partner etc. Terms that are associated with this include pain related fear, fear avoidance, anxiety, stress, depression etc. All this has an impact on a person’s ability to cope. The overarching term used to refer to this reduction in activity levels is pain related disability. A misconception related to this term is that if someone has high disability, and they have high pain, there must be a causal link between pain and disability. That pain causes disability and if you can reduce the pain, you can reduce disability. Unfortunately, this can lead to treatment approaches with a strong focus on pain reduction resulting in an increase in worry (Eccleston & Crombez, 2007), and reduced attention to the factors that are associated with the person seeking treatment or the challenges they face in decreasing their disability (Jones, Grimmer, Edwards, Higgs, & Trede, 2006). Treatments with a focus on a reduction on pain can lead to an increased lack of control or “external locus of control”and a decrease in a person’s confidence to manage the factors that are associated with disability (see fig.1).
What is locus of control?
Locus of control refers to the belief that a person can control the outcome of the situation. Quite simply, people living with pain with internal locus of control can be described to have a good ability to cope and fall upon management strategies to help them through a period of pain adversity (Thompson, 2015). That they have control of their destiny despite pain. Whereas, someone with external locus of control is likely to have a reduced ability to cope because no matter what the person does bad things continue to happen outside of their control, often seeking out help from others. Now that doesn’t mean it’s a bad thing because perhaps the person needs support to lose weight or to update their sense-making of pain. It’s when the person lacks confidence in their ability to act towards making a change and so continues to seek out repeat pain reduction treatments.
What is self-efficacy?
Self-efficacy is based on Social learning theory by Albert Bandura, (1997). It is defined as ”people’s beliefs about their capabilities to produce designated levels of performance that exercise their influence over events that affect their lives”
Self-efficacy influences our thoughts, emotions, actions and motivations and plays a crucial role in shaping our perception of life experiences. If we have previously encountered negative life-experiences it can affect the valence we place upon current and future situations. In the case of pain this might present as pain related fear or anxiety.
Consider someone who lacks the confidence when performing an action or task due to the belief that further damage will occur as a result of pain experienced in the past, or that they’ve been given an understanding from, say healthcare professionals that hurt is equal to harm.
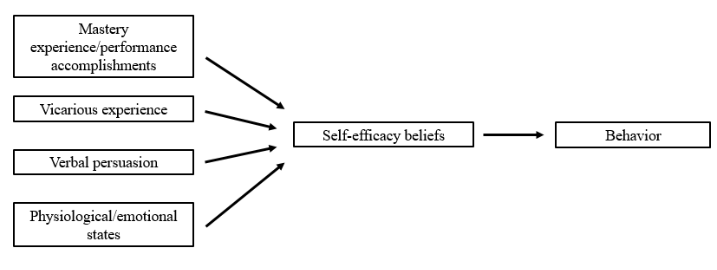
The theoretical concepts of self-efficacy according to Bandura (1997) include Mastery experiences, verbal persuasions, social modeling or vicarious experiences, and emotional and physiological states (See Fig 2). Healthcare professionals play a huge part in taking on the role of supporting these concepts.
Mastery experiences is best described as the experiences we gain when we succeed at the challenges we take on. For example, sticking to the rules of the Covid-19 outbreak to minimize your risk of transmission and infection. Reading the information is not enough. Acting and adhering to the rules is when we are more likely to feel we have succeeded. Fordyce’s popular phrase ‘For behavior change, information is like wet noodles to a brick’ is a wonderful metaphor to explain how being educated is not enough for behavior change we need to practice activities and tasks for true success. Many recent articles have highlighted the importance of education and exercise including the recent Back Pain series in the Lancet (Foster et al., 2018). At the same time we need to believe that we can accomplish the task as this will also positively influence our behavior.
Verbal Persuasions describe how words can positively impact a person’s self-efficacy. Having someone that we can talk to, or that inspires us and acts as a role model. Words of encouragement and positive reinforcement can be very motivating towards our willingness to succeed.
Vicarious experiences or observational learning is a hugely important aspect of building self-efficacy. Seeing other’s successfully performing activities that may be deemed threatening can help observers generate expectations that they too will improve if they persist in their efforts. Through building a therapeutic relationship of trust, openness and empathy healthcare professionals can often take the place of a role model. This means that our demonstrations of movements and exercises are important, with little emphasis on correct technique and more on the “can do it”rather than the “can’t do it”.
Finally, emotional and physiological states refer to how context plays a role in overall health and well-being. It’s important to consider the factors that may be involved for why someone might present with stress or anxiety or worry. When people are struggling with these emotional and physiological states it can be difficult to have a healthy level of well-being and hard to boost self-efficacy.
A term that jumps to my mind here is flexible persistence. Taken from Acceptance and Commitment Therapy literature, flexible persistence is about finding ways to achieve the end result – doing what you love – but using anything and everything to help you get there. Consider the self-efficacy concepts above and you can see how they tie in nicely with flexible persistence.
Self-efficacy has been widely studied in pain research, particularly the effect it has on functional outcomes (reference). Pain self-efficacy is defined as the patients’ confidence in his or her ability to tolerate pain and perform daily activities or to achieve a desired outcome, despite their pain. Higher levels of self-efficacy have been found to be associated with lower levels of pain and disability (pain interference) in patients with chronic pain (Karasawa et al., 2019; Nicholas, Lintion, Watson, & Main, 2011).
Why is self-efficacy so closely tied to goal setting?
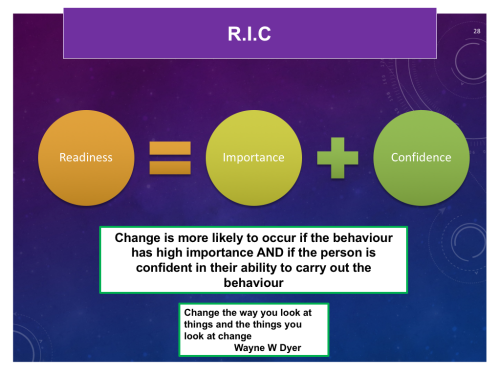
Well, self-efficacy is more to do with the belief in a person’s ability to go through the steps necessary to produce a desired outcome. Personal goal – setting is influenced by self-appraisal of capabilities. it is an important behavior change technique. Goal setting asks if the person believes or has confidence in their ability to perform a task. The stronger the perceived self-efficacy, the higher the goals people set for themselves, the more likely they will achieve them and the firmer their commitment. In order for an individual to demonstrate readiness for change the goal has to be of high importance to the person and the person needs to have high confidence that they can achieve the goal (see fig.3).
But what about people living with pain who report high levels of pain intensity, high levels of disability and low self-efficacy but say, “I want to return to work.”
Whilst this may seem like an appropriate goal for people, the clinician should investigate how the person intends to achieve this goal. By remaining curious at all times, we can tease out valuable information that can help us to guide and thus facilitate a direction towards the desired outcome. The conversation might go something like this:
Therapist:“I’d like to explore some things that are meaningful or important to you and set some goals around that if we can. Are you happy to discuss the things that give you meaning in your life that you would like to work towards?”
Client:“All I want is to return to work. I’m tired of sitting around at home”
Therapist:“I can see that returning to work is important to you. I respect and admire your motivation for wanting to return to work. May I ask what’s important about going back to work and what might going back to work look like? What’s the next best step?”
Client:“Going back to work would mean that I can earn some money and by presents for my kids. I’m not sure what the next best step is? What I do know is if I can get rid of my pain then I can go back to work.”
Therapist:“Yes I understand, pain can be such a hindering and frustrating thing that just gets in the way of what we want to do in life. It can even get in the way of trying to achieve the steps to success and that can even be before you get started! Tell you what, would you be willing to lay out some steps with me towards achieving your goal?
We can see that the client has a strong desire to return to work, however they may not have thought about the steps to get there. It is often the case that vague or unrealistic goals can be expressed particularly if pain reduction measures have failed. It can be easy when living with chronic pain to over-focus on losses which can have a negative effect on mood and activity levels.
The important parts from my perspective are the following - we increase self-efficacy by setting up situations where behavioral successes can occur. When people get success, they feel more self-efficacious, which increases the probability of continued success.
We cannot start or end with self-efficacy alone. We must describe the conditions by which that experience influences behavior and the conditions by which our treatments can increase that experience.
It’s like any cognitive event - positive thinking, catastrophizing, acceptance, etc. We cannot stop the analysis by concluding that any private event (a thought, feeling, or sensation) is “good” – it’s useless to stop at that point as it does not specify the conditions above. It’s important to consider how experiences influence behaviour – Fordyce’s metaphor!
So how might we work on self-efficacy in practice?
Pain Self-Efficacy is closely associated with fear of movement. Therefore we need to analyse and understand how current coping methods are tied to a person’s beliefs about the task or movement - do they avoid it and why? We should then discuss and identify with the client whether the coping methods and beliefs are helpful or unhelpful - do they work towards or away from what’s important to them? Based on this information we would then generate an agreed hierarchy of personalised activities the person feels are important to them and/or is concerned about - steps to success. We could then use graded activity and graded exposure to increase confidence in movement and activity levels - consider the concepts of self-efficacy above, savour the moments of success.
To sum up
What is self-efficacy? It’s not enough for us to know that self-efficacy is good. We must identify its qualities AND treatment modalities that seek to increase it.
So - self-efficacy is the belief that I have the ability to influence my environment (internal - thoughts, feelings, memories and external - what we see, smell, hear, touch, taste).
Then, we need to describe why more self-efficacy is better. Then, we need to be able to identify how to increase self-efficacy in ourselves/our clients.
For example, I believe that I can keep active each day during these pandemic times (self-efficacy). The belief that I can keep active means I am more likely to keep active. I can increase that belief by proving to myself that I can keep active. The ways that I can keep active are to get up at the same time each morning and go for a run with my partner. Each day that I do that, I increase my self-efficacy and hopefully my partners too!
BUT, the point is that it’s going on the RUN that increases self-efficacy. One could argue that the process starts with the run, not with the feeling.
Thanks for having a read
TNP
References
Bandura, A. (1997). Self-efficacy. The exercise of control.(D. of E. S. Emory University & I. on S.-E. A. C. of S. Dies, Eds.). New York: W.H.Freeman and Company.
Eccleston, C., & Crombez, G. (2007). Worry and chronic pain : A misdirected problem solving model. Pain,132(3), 233–236. https://doi.org/10.1016/j.pain.2007.09.014
Foster, N. E., Anema, J. R., Cherkin, D., Chou, R., Cohen, S. P., Gross, D. P., … Woolf, A. (2018). Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet, 391(10137), 2368–2383. https://doi.org/10.1016/S0140-6736(18)30489-6
Jackson, T., Wang, Y., Wang, Y., & Fan, H. (2014). Self-efficacy and chronic pain outcomes: A meta-analytic review. Journal of Pain, 15(8), 800–814. https://doi.org/10.1016/j.jpain.2014.05.002
Jones, M., Grimmer, K., Edwards, I., Higgs, J., & Trede, F. (2006). Challenges in applying best evidence to physiotherapy practice: Part 2 - Health and clinical reasoning models to facilitate evidence-based practice. The Internet Journal of Allied Health Sciences and Practice, 4(4).
Karasawa, Y., Yamada, K., Iseki, M., Yamaguchi, M., Murakami, Y., Tamagawa, T., … Inada, E. (2019). Association between change in self-efficacy and reduction in disability among patients with chronic pain. PLOS ONE, 14(4), e0215404. https://doi.org/10.1371/journal.pone.0215404
Nicholas, M. K., Lintion, S. J., Watson, P. J., & Main, C. J. (2011). Early Identification and Management of Psychological Risk Factors (“Yellow Flags”) in Patients With Low Back Pain: A Reappraisal. Psychologically Informed Practice, 91(5), 737–753.
Thompson, B. L. (2015). Living well with chronic pain : A classical grounded theory. https://doi.org/10.13140/2.1.4141.3923

1 Comment