Hi all welcome to another naked tales of a studying physio. Here’s the first part of my second assignment for my post-graduate studies. It’s a back pain case study about a thoracic disc herniation and calcification. A small note before you read on. There is minimal evidence (very low quality) (all case studies) that show thoracic disc calcification or calcific discitis in adults (as I understand it is also called) (what do we know about medical terminology? Just causes confusion) cause myelopathy. Furthermore, it appears that most massive thoracic disc herniations with calcific discitis spontaneously regress (Xu, Wei, Liu, Jiang, & Liu, 2016). Just the body’s way of adapting as best it can.
Introduction
Epidemiological studies show that chronic, widespread, nonspecific musculoskeletal pain, particularly back pain, continues to be a growing problem the world over (Hoy et al., 2012; McBeth & Jones, 2007; Yelland, 2011). Disability associated with back pain has a higher prevalence than any other health condition (Hoy et al., 2014). Back pain is reported to have a higher prevalence in years lived with disability than cancer, heart disease and diabetes (Vos et al., 2012), and it has an observable effect on care-seeking, disability, activity avoidance and social withdrawal (Linton, 2000; Ramond et al., 2011).
Back pain has traditionally been treated through biomedical approaches including physiotherapy, complementary therapies, medication, injection and surgery at an increasing cost to healthcare. Single approaches such as these aim to treat pain and disability, however, the evidence does not show this to be efficacious (Kamper et al., 2015; Walsh & Radcliffe, 2002). As a result, back pain related disability continues to grow at an alarming rate (Deyo et al., 2009; Hoy et al., 2012; Lin & O’Sullivan, 2014).
Approaches such as passive therapies, injection therapy and surgery are commonly recommended by clinicians and regarded by the public as means of pain management despite their limited effectiveness in the long term (Deyo et al., 2009; Chou et al., 2007; Armon et al., 2007; Clark et al., 2011; Kumar, Beaton, & Hughes, 2013; Nijs et al., 2013). It is important to understand why this is the case. The driving force behind this thinking are the outdated views of Cartesian philosophy and other theories (specificity theory and summation theory) proposing that there is a separation between mind and body, creating the misconception that the body is a machine (Skelton, Wearn, & Hobbs, 2002). This has enabled the biomedical model to thrive, as the notion that signs and symptoms arise from structural or functional abnormalities that need fixing. Furthermore, this legacy of inaccurate beliefs compounded by crude terminology (such as waterworks to describe the urinary system or mechanical to describe movement of the musculoskeletal system), has perpetuated a public misconception about ‘faulty parts’ causing pain and damage that therefore requiring ‘fixing’ in order to be able to function (Darlow et al., 2013; Hoffmann et al., 2013; Liddle, Baxter, & Gracey, 2007).

Figure 1. Image to illustrate the affect language can have on pain and disability
In terms of back pain, a belief in the fragility of the spine appears to have manifested in the public as a result of this mechanistic understanding and ‘quick fix’ approach (O’Keeffe et al., 2015). Additionally, literal or metaphorical language about the body as a machine and poor communication between clinician and patient can have a compounding effect, perpetuating the person’s beliefs about the injury (Barker, Reid, & Minns Lowe, 2009, 2014; Greville-Harris & Dieppe, 2015).
The following case study is an example of the ongoing beliefs that seem to be held by many clinicians and the general public regarding causal links between pain and pathology, and how language can influence fear associated with pathology, eventually leading to disability. A case formulation process follows the case study to aid clinical reasoning for intervention application and goal setting.
Case Description
The patient was seen at a physiotherapy clinic in Auckland. The patient signed a consent form agreeing to participate in a case formulation of a single case study.
Presentation
The patient is a 56-year-old male who presented for the functional component of a comprehensive pain assessment as part of a reopened ACC claim. The patient, a used car salesman, fell from his bicycle whilst cycling through a part of Auckland city on the 28th of October 2011. The ambulance crew noted that the patient was intoxicated and taken to Auckland City Hospital. An x-ray identified multiple fractures of the patient’s spine at spinal levels C1/C2/T4 - T7 and multiple rib fractures, including the first rib bilaterally. The patient also suffered a mild traumatic brain injury and was treated by concussion services as a result of post-concussion symptoms. A neurological assessment identified executive dysfunction issues.
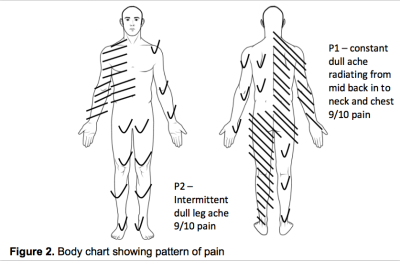
The patient reported that his main pain was located in the middle of his back with a radiation of intermittent sharp stabbing pain into the right side of his rib cage up into his neck and head and intermittently into his left leg. The patient indicated on a body chart (see Fig. 2) the location and behaviour of his symptoms, and with the widespread distribution of the symptoms he experienced, it appeared consistent with a central sensitization presentation. The pain into the ribcage caused a restriction in his breathing as it hurt to breath diaphragmatically. He explained that it felt like he was “being crushed in a vice” and that the pain in his back was like “a dog sinking its teeth into my back.” There was no relief in his pain, as he reported that it ranged from a 4/10 (controlled with medication) to a 9/10 on a numerical pain rating scale. He also reported pain into his right arm particularly when performing overhead activities. The patient stated that his symptoms became worse with increasing activity and he was in more pain by the end of the day (if he had attempted several domestic activities of daily living (ADLs)). His symptoms were relieved if he lay down on his back.
Lets leave it there for Part 1. Part 2 will be with you next week and will give more insights into the biopsychosocial factors that were involved in this case. The beliefs and behaviours in particular are particularly interesting.
Thanks for having a read
TNP
References for all parts
Armon, C., Argoff, C. E., Samuels, J., & Backonja, M.-M. (2007). Assessment: use of epidural steroid injections to treat radicular lumbosacral pain. Neurology, 68, 723–729. http://doi.org/10.1212/01.wnl.0000256734.34238.e7
Barker, K. L., Reid, M., & Minns Lowe, C. J. (2009). Divided by a lack of common language? A qualitative study exploring the use of language by health professionals treating back pain. BMC Musculoskeletal Disorders, 10, 123. http://doi.org/10.1186/1471-2474-10-123
Barker, K. L., Reid, M., & Minns Lowe, C. J. (2014). What does the language we use about arthritis mean to people who have osteoarthritis? A qualitative study. Disability and Rehabilitation, 36(5), 367–372. http://doi.org/10.3109/09638288.2013.793409
Borg, G. A. (1982). Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise, 14(5), 377–381. http://doi.org/10.1249/00005768-198205000-00012
Chou Roger , MD; Qaseem Amir , MD, PhD, MHA; Snow Vincenza , MD; Casey Donald , MD, MPH, MBA; Cross Jr J. Thomas ., MD, MPH; Shekelle Paul , MD, PhD; and Owens Douglas K. , MD, M. (2007). Clinical Guidelines Diagnosis and Treatment of Low Back Pain : A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society, (July 2007).
Clark, B. C., Goss, D. A., Walkowski, S., Hoffman, R. L., Ross, A., & Thomas, J. S. (2011). Neurophysiologic effects of spinal manipulation in patients with chronic low back pain. BMC Musculoskeletal Disorders, 12, 170. http://doi.org/10.1186/1471-2474-12-170
Darlow, B., Dowell, A., Baxter, G. D., Perry, M., Mathieson, F., Perry, M., & Dean, S. (2013). The Enduring Impact of What Clinicians Say to People With Low Back Pain. Annals of Family Medicine, 11(6), 527–534. http://doi.org/10.1370/afm.1518.INTRODUCTION
Deyo, R. a, Mirza, S. K., Turner, J. a, & Martin, B. I. (2009). Overtreating chronic back pain: time to back off? Journal of the American Board of Family Medicine : JABFM, 22(1), 62–68. http://doi.org/10.3122/jabfm.2009.01.080102
Eccleston, C., & Crombez, G. (2007). Worry and chronic pain : A misdirected problem solving model. Pain, 132(3), 233–236. http://doi.org/10.1016/j.pain.2007.09.014
Ferreira, M. L., Machado, G., Latimer, J., Maher, C., Ferreira, P. H., & Smeets, R. J. (2010). Factors defining care-seeking in low back pain - A meta-analysis of population based surveys. European Journal of Pain, 14(7), 747.e1–747.e7. http://doi.org/10.1016/j.ejpain.2009.11.005
Greville-Harris, M., & Dieppe, P. (2015). Bad is more powerful than good: The nocebo response in medical consultations. American Journal of Medicine, 128(2), 126–129. http://doi.org/10.1016/j.amjmed.2014.08.031
Hoffmann, T., Del Mar, C., Strong, J., & Mai, J. (2013). Patients’ expectations of acute low back pain management: implications for evidence uptake. BMC Family Practice, 14(1), 7. Retrieved from http://www.biomedcentral.com/1471-2296/14/7
Hoy, D., Bain, C., Williams, G., March, L., Brooks, P., Blyth, F., … Buchbinder, R. (2012). A systematic review of the global prevalence of low back pain. Arthritis and Rheumatism, 64(6), 2028–2037. http://doi.org/10.1002/art.34347
Hoy, D., March, L., Brooks, P., Blyth, F., Woolf, A., Bain, C., … Buchbinder, R. (2014). The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Annals of the Rheumatic Diseases, 73(6), 968–974. http://doi.org/10.1136/annrheumdis-2013-204428
Kamper, S. J., Apeldoorn, A. T., Chiarotto, A., Smeets, R. J. E. M., Ostelo, R. W. J. G., Guzman, J., & van Tulder, M. W. (2015). Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ (Clinical Research Ed.), 350(February), h444. http://doi.org/10.1136/bmj.h444
Kumar, S., Beaton, K., & Hughes, T. (2013). The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews. International Journal of General Medicine, 6, 733–41. http://doi.org/10.2147/IJGM.S50243
Liddle, S. D., Baxter, G. D., & Gracey, J. H. (2007). Chronic low back pain: patients’ experiences, opinions and expectations for clinical management. Disability and Rehabilitation, 29(776008562), 1899–1909. http://doi.org/10.1080/09638280701189895
Linton, S. J. (2000). A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976), 25(9), 1148–1156. http://doi.org/10.1097/00007632-200005010-00017
McBeth, J., & Jones, K. (2007). Epidemiology of chronic musculoskeletal pain. Best Practice & Research. Clinical Rheumatology, 21(3), 403–25. http://doi.org/10.1016/j.berh.2007.03.003
Nijs, J., Roussel, N., van Wilgen, P. C., Koke, A., & Smeets, R. (2013). Thinking beyond muscles and joints: Therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Manual Therapy, 18(2), 96–102. http://doi.org/10.1016/j.math.2012.11.001
O’Keeffe, M., Purtill, H., O’Sullivan, P., Dankaerts, W., Conneely, M., Hurley, J., … O’Sullivan, K. (2015). Comparative effectiveness of active interventions for non-specific chronic spinal pain: Physical, behavioural or combined? A systematic review and meta-analysis. Physiotherapy (United Kingdom), 101, eS1131–eS1132. http://doi.org/10.1016/j.jpain.2016.01.473
Ramond, A., Bouton, C., Richard, I., Roquelaure, Y., Baufreton, C., Legrand, E., & Huez, J. F. (2011). Psychosocial risk factors for chronic low back pain in primary care-a systematic review. Family Practice. http://doi.org/10.1093/fampra/cmq072
Skelton, J. R., Wearn, A. M., & Hobbs, F. D. R. (2002). A concordance-based study of metaphoric expressions used by general practitioners and patients in consultation. British Journal of General Practice, 52(475), 114–118.
Sullivan, M. J. L., Bishop, S. R., & Pivik, J. (1995). The Pain Catastrophizing Scale: Development and validation, 7(4), 524–532. Retrieved from http://www.scopus.com/inward/record.url?eid=2-s2.0-0029584617&partnerID=40&md5=7f8615d1b52cbabde152c2e9b9683fff
Tait, C.R. Pollard, C.A. Margolis, R.B. Duckro, P.N. Krause, S. J. (1987). The Pain Disability Index: Psychometric and Validity Data. Archives of Physical Medicine and Rehabilitation.
Thomas, E. N., Pers, Y. M., Mercier, G., Cambiere, J. P., Frasson, N., Ster, F., … Blotman, F. (2010). The importance of fear, beliefs, catastrophizing and kinesiophobia in chronic low back pain rehabilitation. Annals of Physical and Rehabilitation Medicine, 53(1), 3–14. http://doi.org/10.1016/j.rehab.2009.11.002
Vertue, F. M., & Haig, B. D. (2008). An Abductive Perspective on Clinical Reasoning and Case Formulation. Journal of Clinical Psychology, 64(9), 1046–1068. http://doi.org/10.1002/jclp
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., … Moradi-Lakeh, M. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2163–2196. http://doi.org/10.1016/S0140-6736(12)61729-2
Walsh, D. A., & Radcliffe, J. C. (2002). Pain beliefs and perceived physical disability of patients with chronic low back pain. Pain, 97(1-2), 23–31. http://doi.org/10.1016/S0304-3959(01)00426-2
Xu, N., Wei, F., Liu, X., Jiang, L., & Liu, Z. (2016). Calcific discitis with giant thoracic disc herniations in adults. European Spine Journal, 1–5. http://doi.org/10.1007/s00586-016-4402-y
Yelland, M. (2011). What do patients really want to know? International Musculoskeletal Medicine, 33(1), 1–2.

1 Comment