
Our clinical practice should demonstrate a good mix of acquired knowledge, clinical experience and supporting evidence. The person seeking care expects to receive a well-reasoned intervention hypothesis that answers questions or concerns, and delivers effective management.
So, evidence based medicine appears to be cropping up everywhere at the moment. That’s not inherently a bad thing, as it’s necessary to be using an evidence based approach to support our clinical delivery. Yet more and more discussions about the use of evidence appear to sway towards confirmation bias in support of clinical beliefs. This concerns me, because as I highlighted recently, this can end up becoming an inter-professional pissing contest.
Let me give you an example. A physiotherapist contributes to a newspaper article about how certain exercises can cause more harm. Particular language is used in the article that is recognised (by many) as unhelpful in that it may be interpreted in a literal sense. The article makes a blanket recommendation that the general public must be vigilant about avoiding these exercises. Can you think what the implications are here?
The same article is then branded by other physiotherapists as fear mongering and misrepresentative of correlation to causative links between exercise and pathology. Can you think of what the implications are here?
Now before you all jump down my throat, I will be the first to hold my hand up and point out the blogs that I have written here and here regarding the use of poor language. Hence this latest blog post is a reflection of my own personal growth and critical thinking.
Adam Meakins @adammeakins recently posted on facebook a great little pyramid, which I think fits in with this blog post.
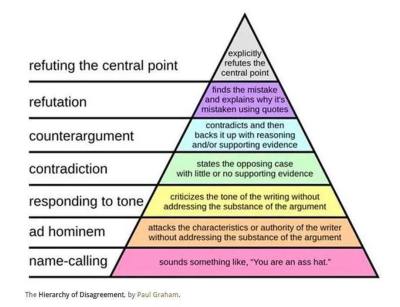
Thinking critically, I would address the same situation like this. Consider the newspaper article and find the evidence that supports the argument for avoiding the exercises that are highlighted in the article. Secondly, identify the evidence that supports the arguments against avoiding the exercises highlighted in the article. Finally, be able to sit and reason the evidence collaboratively with your audience. This way of reasoning is a simple CBT approach, very effective for providing a balanced view of the available information.
Just because a newspaper article makes a blanket recommendation about certain exercises being bad for you, is it not just as bad to accuse the article of fear-mongering? We are all trying to do what’s best by our patient. If we continue to engage in pissing contests within our own profession, not only do we become our own nemesis, but we show the public that there is disunity within our profession. Ultimately, we lose trust from the people we are trying to help. I am faced with more and more disgruntled patients about their lack of trust in the physiotherapy profession because of the exact situation given above.
I ask all clinicians to consider the implications of our actions in and outside of clinical practice and the repercussions to ourselves as well as the profession in its entirety.
Thanks for having a read
TNP
