
You’re on the court playing the best game of your life, everything is coming together, the silky skills, the shimmy, your sprinting down the line and you tumble in a heap to the ground holding your ankle! Was it a sniper? (common football chant) did you lose your footing?, was it the shiny floor that took you out? Your team mates are being less than helpful shrugging their shoulders whilst you’re holding your painful ankle! In a split second questions start looming, what have I done? Is it serious? Will I play like Michael Johnson again? No-one likes a swollen ankle, they look unpleasant, they hurt, throb, ache and it can seem to take ages for them to get better, so you know what let’s talk about ankle sprains…….Yay! I hear you all cry with excitement!
Introduction
Ankle sprains are very common, spraining the ligaments on the outside of the ankle (inversion ankle sprain) are more common than the inside, so I will focus this post on the lateral ligaments of the ankle. Ligament structures are pretty tough so you have to do a lot to damage them. An ankle sprain can do just that having a significant effect on time off work particularly if severe and left untreated, 40% of which result in chronic instability (reference). As with all my posts if you sustain an injury don’t delay get it seen right away!
Anatomy
Let’s take a look at the anatomy of the outside of the ankle to identify what structures are commonly involved with an inversion ankle sprain.
.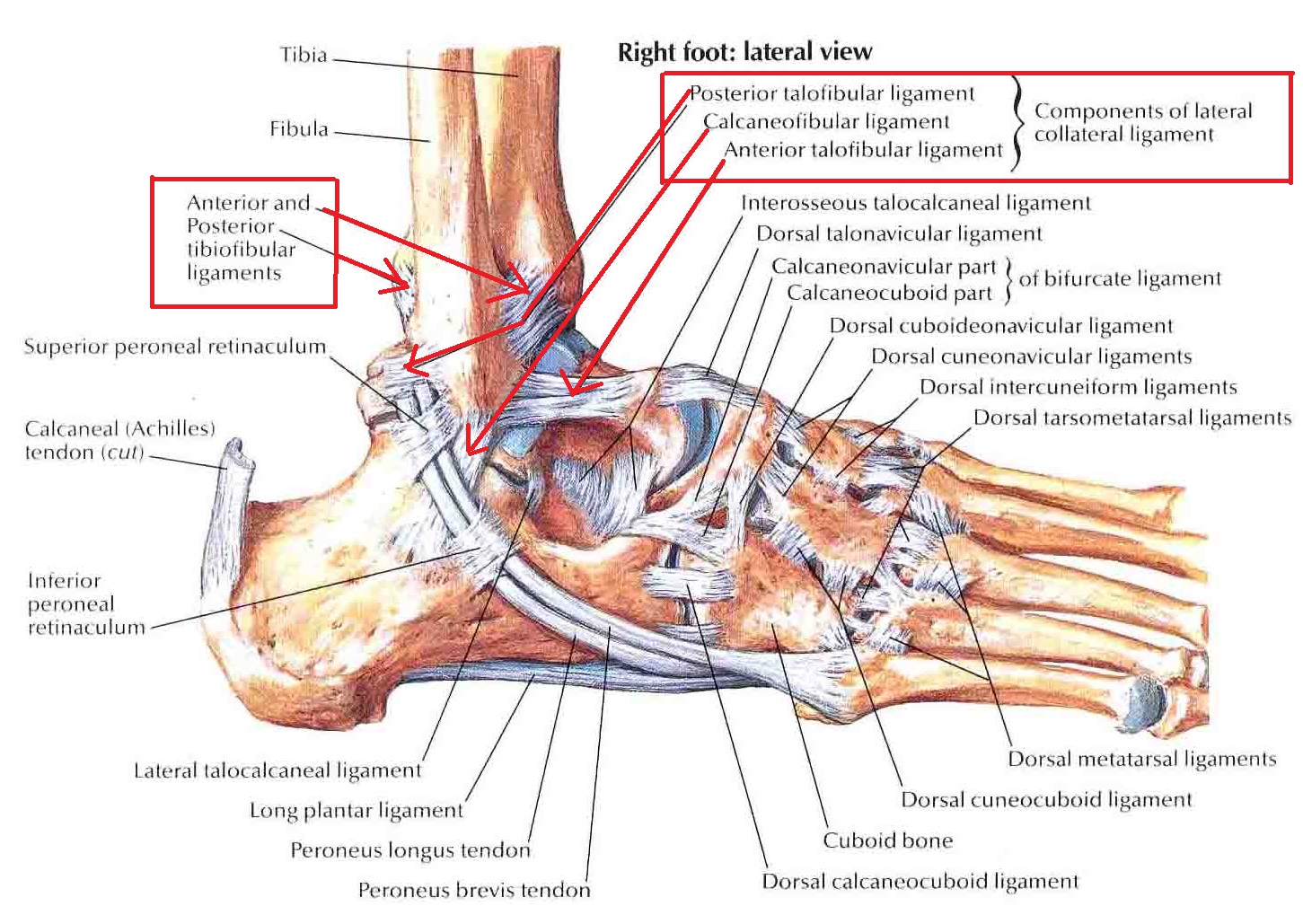
The lateral ligaments are highlighted in red including the Anterior Talofibular Ligament (ATFL) most commonly injured and is part of the anterior capsule so will swell when is injured, this is most likely the reason why you get that fat ankle appearance as the ligament is relatively weak. The Calacaneo-fibular Ligament (CFL) and the Posterior Talofibular Ligament (PTFL) make up the remainder of the lateral ligament complex. They are thicker and stronger and play more of a role in stability of the ankle joint. The ATFL has a 90% hit rate in inversion ankle sprains. So when you sprain your ankle it is highly likely that you will have injured this ligament. Other structures include the talus (talar dome fracture) the navicular bone, the 5th metatrsal, peroneal tendons and surrounding sheaths, sinus tarsi and with repeated ankle sprains can lead to ankle instability.
Causes of injury
The lateral ligaments of the ankle are vulnerable to inversion type movements such as a trip off a curb or (having worked in netball) landing on an opponents foot from a jump and going over your ankle. The ligaments, peroneal tendons and intrinsic muscles groups are all susceptible. A set of examination procedures called the Ottawa rules help to eliminate serious pathology like a fracture for example. The rules go more into detail about the procedures but to simplify it: if you are unable to weight bear after a 48 hour period it is important that you get your ankle seen too in order to rule out a fracture (reference). It may not be necessary to get an x-ray within that time. Another sign is the degree of swelling, if there is a large amount of swelling then it is likely that you may have sustained a fracture, however the prevalence of fractures is less than 15%. Again the advice here is if you do experience any of the above it’s best to get it checked out.
Classification
The severity of an ankle sprain can be graded accordingly - Mild (grade 1) Moderate (grade 2) Severe (grade 3) (reference)
Mild sprain (grade 1):- Classified as a stretch of the ligament without macroscopic tearing, little swelling or tenderness, slight or no functional loss, and no mechanical instability of the joint. These sprains tend to occur in the same mechanism as moderate and severe tears but with little disruption of tissue. It is best to use the POLICE acronym (see report here) to manage this with a gradual return to running as function returns. Balance and strength training may be of help to facilitate recovery.
Moderate sprain (grade 2):- A grade 2 injury is a partial macroscopic tear of the ligament with moderate pain, swelling, and
tenderness over the affected structures. Some loss of motion and mild or moderate instability. This can be variable depending on the degree of swelling which often indicates the degree of tissue insult. I’ll admit grading of sprains can be difficult hence if there is considerable swelling and it is difficult to weight bear after 48 hours it is best to get an x-ray.
Severe sprain (grade 3):- There is complete rupture of the ligament with severe swelling, haemorrhage, and tenderness. There is loss of ability to bear weight on the foot, limited function, and considerable abnormal motion and instability of the joint. An anterior draw test of the ankle and talar tilt test will be positive. As highlighted by the Ottawa rules it is best to pop yourself off to A&E or your GP to get this checked out.
Management
Lets look at the management of ankle sprains considering the use of bracing and optimal loading. Mild sprains usually cause minimal disruption to tissue and there is minimal time required to be away from your sport. If there is then you may have sustained a more severe injury.
When tissue disruption is involved you will expect to see considerably more swelling, which indicates more tissue damage. If you have had an x-ray that has ruled out a serious pathology such as a fracture you can begin to load the tissue in a gradual way. You may be issued crutches or sometimes placed in a moonboot or be given some of that rubbish tubigrip stuff to help reduce the chances of recurrence of injury. Tubigrip hasn’t really got any strong evidence behind it to support its effectiveness. Ideally you need a lace up brace or semi-rigid brace to provide adequate support and swelling control. Now please don’t go into A & E departments demanding they should give you a lace up brace when you sprain your ankle because it just won’t happen. Speak to your physio to help you recommend an appropriate one for you. The evidence suggests that immobilisation (4 weeks) over use of functional restoration is detrimental to recovery. A short period of immobilisation of up to 10 days can help to control pain and swelling (reference). However I would advise gently moving your foot in this time as pain allows, managing appropriately with POLICE. Crutches are actually quite important as they facilitate recovery by encouraging correct tissue healing, maintain proprioception and help to restore confidence (reference, reference).
Ligament injuries can take up to 12 weeks to heal depending on the severity of the injury. So being mindful of the above advice will help in your recovery. This will also help to reduce a recurrence of an injury to the ankle. All too often we tend to rush back to our specific activity or sport. This is either due to peer pressure, fear of deconditioning, eagerness to return, social isolation, not making the team etc. The body needs time to heal, rushing this process will not bring you any favours. So avoid any high level activity, jumping, running etc. Long walks can also cause you discomfort in the initial stages of healing. In the first 4 weeks after injury the tissue is fragile and is going through a repair phase so any high level activity that will stress it is gonna compound the injury and just set you back.
Promoting recovery through diet, appropriate rest/sleep, and following the advice of your clinician can expedite your injury recovery and is recommended. Check out my other posts on advice on eating for a better recovery (here) and injury management (here).
The main aim of management is restore you function as soon as possible. We can break these up into range of movement restoration, regaining muscle strength, improving balance and restoring functional movement. After a short period of immobilisation
Range of Movement
Restoring all ranges are important you can continually assess this by comparing to your non injured ankle. Moving the foot in all directions will help collagen makeup and alignment and help to promote muscle strength throughout the whole of the ankle range. Try and do all movements of the ankle at regular intervals on a daily basis.
Muscle strength
As you are working through range of movement you are also gradually increasing muscle strength, restoring the strength of the peroneal muscles on the outside of your foot is vital as these muscles will have taken a beating as well as the ligaments when you sustained your injury.
Balance
This is another really important part of rehab as you need to be confident that you have good awareness of your foot and that your nervous system can function well to support your foot without you needing to think about it whilst running or playing sport.
Functional strength
It’s also really important to make sure that you progress up to functional exercises as these are the basis of what movements you will need to perform whilst doing your sport or activity. It’s pretty important to do functional exercise as strength training of individual muscles will be of little value if you don’t integrate it into functional training. Functional training may include exercises such as squats - single or double leg, lunges, jumps, hops or bounding type exercises. A lot of us don’t realise the value of doing these types of exercises thinking that doing some stretches and exercise to the injured muscles will be sufficient. Training your nervous system to fire the muscles at the right time during a movement such as running is very important to prevent recurrence.
Return to sport/activity
Sports have a variety of movements and a variety of components of muscle/nervous system function including strength, balance, flexibility, power, endurance, speed, co-ordination, reaction time and so on. This can all be integrated into your rehabilitation program but you need to be sure that you are confident in your ankle that you can perform these components pain free. Your physiotherapist and strength and conditioning coach/Personal Trainer can discuss this all with you.
So hopefully you’ll be back on the field playing like Pele in no time at all! Remember if you injure your ankle or any other limb, it is really important that you get it checked out. Leaving it and thinking it will just go away usually results in further problems. If in doubt get it checked out!
Thanks for having a read. Your comments are welcome here and on thenakedphysio facebook page.
TNP
