Sometimes I wonder why I just don’t ask a simple question such as, “what are safety behaviours?” Oh no, not me I like to ask deeper questions! So, this blog is kind of an opinion piece but more ramblings about reading and interpretation. Apologies in advance if I go off track. Writing is thinking and consolidating knowledge after all!
The fear avoidance model (FAM) without question has provided clinicians working in pain management an opportunity to implement interventions to address aspects of pain including pain related fear, avoidance behavior and disability. Whilst there appears to be an interdependency between fear and avoidance in persistent pain is it worth asking the question:
Is avoidance behavior always related to fear and is it always something that always needs to be extinguished?
Of course I would say yes, because even though the FAM is an amazing conceptual model, to me it still categorises patients into a fear avoidance framework. Now the Vlaeyen and colleagues had always stressed the point the FAM was never intended to be a final model. They welcomed adaptation, development and evolution, but at the same time it was still brilliant for helping individuals that had developed a phobia type presentation to movement, particularly with back pain.
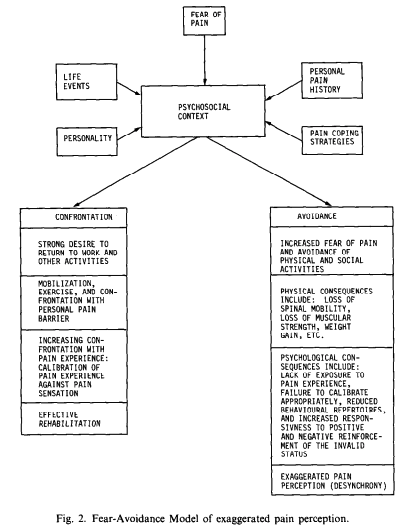
The FAM is well known to be associated with Vlaeyen & Linton, (2000)who published a review of fear avoidance and its consequences in chronic musculoskeletal pain. Yet, the original FAM came from work of Lethem et al (1983) indicating that the ‘fear of pain generates in some individuals a strategy of avoidance rather than confrontation which in turn leads to both physical and psychological reinforcement of the invalid status.’ Whilst research has further developed and progressed the understanding of the fear avoidance model as proposed by Lethem et al (1983), the underpinning of the model is based on the association of two distinct notions, fear and avoidance. Fear is a physiological response to threat or with respect to the FAM, pain, and avoidance (again in this context) is the behavioural response to pain. What research does seem to point at is there is an association between pain intensity and fear avoidance (Kroska, 2016).
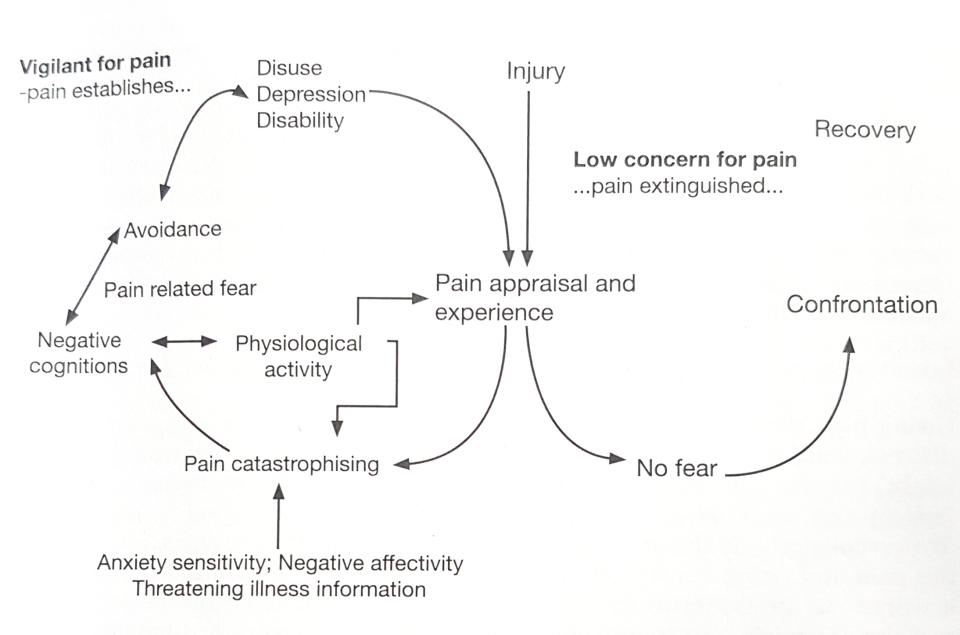
The FAM by Vlaeyen & Linton, (2000) proposed 2 avenues that individuals experience following injury. 1) Pain following an injury is perceived as unpleasant but not catastrophic. As such the individual engages in appropriate behavioural restriction and gradually increases activity towards recovery, or 2) individuals appraise pain as threatening and potentially catastrophic, which can be influenced by negative affect and threatening illness information, resulting in the development of fear of pain leading to avoidance behavior, hypervigilance to bodily sensations, functional disability and depression resulting in a perpetuation of the cycle.
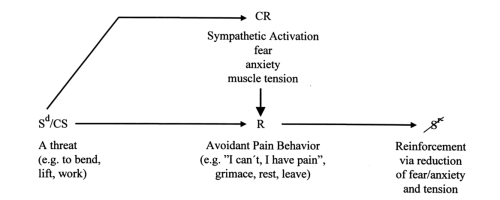
If we consider conditioning models within the FAM there are previous pieces of evidence that also corroborate the FAMs inception. Linton et al, (1984) developed an ‘activity’ avoidance model that captured classical and operant conditioning. Essentially conditioning can occur either through the inciting injury (such as bending to lift a box), negative biomedical information (Don’t bend your back like a crane) or even seeing someone else experience an acute episode of pain (all being an example of a conditioned stimulus). This can lead to a conditioned response – increased muscle tension, fear, anxiety which leads to avoidance behavior, a form of negative reinforcement where something is removed (anxiety, fear of further pain or damage in relation to lifting) to reinforce the behavior, in this case avoidance.
So, with respect to the FAM we can see that the cognitive appraisal or judgement of the injury (eww disaster) can lead to a feeling (fear) and then a behavior (avoidance). However, back to the original question. I’m curious to know if avoidance behavior is always related to fear and is it always something that needs to be extinguished? I mean I might not fear lifting a box but I might still avoid it because it just looks too heavy. Does that mean that I am fearful of it? Or is it because I just don’t have the strength to lift it, so why bother?
Sticking with conditioning models, operant learning is a method of learning that occurs through rewards and punishments for behavior. Avoidance behavior (which is a form of negative reinforcement – see chart) is closely linked with the mechanisms of safety behaviours. Meaning it is an overt action to prevent the occurrence of a feared outcome (Hood, Antony, Koerner, & Monson, 2010; Salkovskis, 1991). So, a safety behavior is a highly effective strategy to minimize or prevent an undesired outcome. Safety behaviours, in the context of pain, may present in various forms including breath holding, grimacing, walking with a limp, use of crutches, keeping your back straight, sitting with good posture etc. Avoidance and escape are also considered safety behaviours so let’s explore each and identify their distinguishing features.
Escape behavior is essentially when someone has committed themselves but then wants to get out of an awkward or painful situation. You’ve all heard of that silly celebrity TV show ‘I’m a Celebrity Get Me Out of Here!’ This gameshow was about pushing people to their limits eating bugs and placing their heads in boxes with creepy crawlies for rewards – a form of perverse positive reinforcement. In order to get out of an increasingly challenging situation (more and more bugs usually) the celebs would say, “I’m a celebrity get me out of here” thus using escape behavior to remove oneself from the aversive stimulus.

In back pain terms the aversive stimulus might be pain whilst picking up the box and so putting the box down would be the escape behavior. One would hope the aversive stimulus then stops. The real problem with musculoskeletal pain is that it is felt within the body. So, how on earth can you escape from that! Many have tried (amputation) and failed. When it comes to pain, as we know can often become persistent (which is where catastrophic thoughts and negative affectivity comes into the FAM). Consequently, escape behavior tends to become avoidance behavior.
Avoidance behavior occurs in anticipation of the aversive stimulus. In the I’m a celebrity example this might be a feeling of yuckiness prior to having their head in a box with bugs resulting in the celeb not doing the challenge at all.
In the back pain example avoidance behavior is an anticipation of pain rather than a response to pain. Avoidance behaviours are incredibly effective because the person receives relief (behavior) from not having experienced the “pain” inducing picking up of a box (removal of a stimulus). This is an example of negative reinforcement under operant learning.
Exposure models are generally tailored to address safety behaviours commonly associated with feelings of anxiety and avoidance behaviour or commonly known as constructs of phobia (Rachman, Radomsky, & Shafran, 2008; Salkovskis, 1991). Those individuals living with pain that display catastrophic tendency’s also display signs of anxiety and concurrently display avoidance behaviour (Carleton, Abrams, Kachur, & Asmundson, 2009; Crombez, Vlaeyen, Heuts, & Lysens, 1999; Sullivan, Bishop, & Pivik, 1995). Whilst working with someone living with persistent back pain, a clinician versed in identifying safety behaviours might view them as something to be extinguished as they are seen to be maladaptive towards an individual’s function (Salkovskis, 1991).
Whilst this would seem logical, a safety behavior may be appropriate for the person to function, which I would consider to be highly dependent on context. So, where a person may adopt a straight back when lifting because it is understood to protect the back from damage, this is a safety behavior. The person (in this case) does not report any pain or fear yet they are still adopting what might be viewed as an avoidance behavior. So, here we can consider the possibility of how conditioning from a classical and operant perspective may change the persons viewpoint of lifting when they experience pain, meaning pain = damage and as such the safety behavior may now be paired in a maladaptive way (Vlaeyen, 2016).
Then take the clinician who also views this behavior as maladaptive and attempts to restore movement with a variability lens. Whereas previously the person was reporting no issues with pain when lifting with a straight back. I consider this to be a conflict of transference between when biomechanics matters and behavioural habits in relation to persistent pain, not forgetting context. Of course this is all speculation on my part and merely some jumbled musings I have on teasing out the similarities between biomechanics and behavioral lenses.
So have I answered my question? Perhaps, Yet a call for further research was recently made in understanding the predictive value of fear and avoidance independently (Kroska, 2016). Furthermore, previous texts have suggested there is no strong relationship between fear and avoidance and some evidence would suggest that avoidance behaviours are fear inhibiting (Asmundson, Vlaeyen & Cormbez, 2004). Finally, research from Pincus, Vogel, Burton, Santos, & Field, (2006)proposed models for social (i.e. health beliefs and health culture policy and familial and close social health beliefs) and psychological (depression) pathways identifying that disuse without fear is linked to avoidance.
Anyway, that’s enough reflections on the FAM. I expect to come back to this blog in the future after reading more on the topic and will likely have more reflections to share.
Thanks for sticking with me this far.
TNP
References
Asmundson GJG, Vlaeyen JWS, Crombez G. Understanding and Treating Fear of Pain. Oxford University Press, NY, USA (2004).
Carleton, R. N., Abrams, M. P., Kachur, S. S., & Asmundson, G. J. G. (2009). Waddell’s symptoms as correlates of vulnerabilities associated with fear-anxiety-avoidance models of pain: Pain-related anxiety, catastrophic thinking, perceived disability, and treatment outcome. Journal of Occupational Rehabilitation, 19(4), 364–374. https://doi.org/10.1007/s10926-009-9191-2
Crombez, G., Vlaeyen, J. W. S., Heuts, P. H. T. G., & Lysens, R. (1999). Pain-related fear is more disabling than pain itself: Evidence on the role of pain-related fear in chronic back pain disability. Pain. https://doi.org/10.1016/S0304-3959(98)00229-2
Hood, H. K., Antony, M. M., Koerner, N., & Monson, C. M. (2010). Effects of safety behaviors on fear reduction during exposure. Behaviour Research and Therapy, 48(12), 1161–1169. https://doi.org/10.1016/j.brat.2010.08.006
Kroska, E. B. (2016). A meta-analysis of fear-avoidance and pain intensity: The paradox of chronic pain. Scandinavian Journal of Pain, 13, 43–58. https://doi.org/10.1016/j.sjpain.2016.06.011
Lethem, J., Slade, P. D., Troup, J. D. G., & Bentley, G. (1983). Outline of a fear-avoidance model of exaggerated pain perception-I. Behaviour Research and Therapy, 21(4), 401–408. https://doi.org/10.1016/0005-7967(83)90009-8
Pincus, T., Vogel, S., Burton, A. K., Santos, R., & Field, A. P. (2006). Fear avoidance and prognosis in back pain: A systematic review and synthesis of current evidence. Arthritis and Rheumatism, 54(12), 3999–4010. https://doi.org/10.1002/art.22273
Rachman, S., Radomsky, A. S., & Shafran, R. (2008). Safety behaviour: A reconsideration. Behaviour Research and Therapy, 46(2), 163–173. https://doi.org/10.1016/j.brat.2007.11.008
Salkovskis, P. M. (1991). The Importance of Behaviour in the Maintenance of Anxiety and Panic: A Cognitive Account. Behavioural Psychotherapy, 19(1), 6–19. https://doi.org/10.1017/S0141347300011472
Sullivan, M. J. L., Bishop, S. R., & Pivik, J. (1995). The Pain Catastrophizing Scale: Development and validation, 7(4), 524–532. Retrieved from http://www.scopus.com/inward/record.url?eid=2-s2.0-0029584617&partnerID=40&md5=7f8615d1b52cbabde152c2e9b9683fff
Vlaeyen, J. W. S. (2016). The intricate relationship amongst pain intensity, fear and avoidance. Scandinavian Journal of Pain, 13, 128–129. https://doi.org/10.1016/j.sjpain.2016.08.010
Vlaeyen, J. W. S., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain, 85(3), 317–332. https://doi.org/10.1016/S0304-3959(99)00242-0

I think the best way to get a baby bird to fly out of the nest is not to scare it out, or tip the nest, but to introduce it to another baby bird who has joyfully discovered what it’s wings were made for.
LikeLiked by 1 person
What a beautiful metaphor, Susan
LikeLike