
Exercise is routinely advocated by healthcare professionals as a treatment to address pain and tissue injury. The consensus that strengthening the local tissue will attenuate pain by improving its resilience whilst transitioning through a natural cycle of tissue healing. Whilst exercise does have morphological effects on local muscle it is understood that increases in muscle hypertrophy at early stages of resistance training are a result of enhanced motor neuron firing and corticospinal excitability (Folland & Williams, 2007). So in the early stages are we really targeting muscle hypertrophy? Another question comes from this. Is it really muscle hypertrophy we want to focus on for people living with pain? That’s probably for another blog.
Exercise is often reported to be painful particularly when working on the affected limb, thus reducing the motivation for exercise adherence. Exercise induced hypoalgesia (EIH) or endogenous analgesia is a popular area of investigation in the research literature and has been advocated as a means to modulate pain following exercise (Bement & Sluka, 2016).
EIH is the phenomenon that occurs following exercise found to reduce pain sensitivity (Bement & Sluka, 2016). Therefore, healthcare professionals can clinically reason that exercise is a means of addressing muscle hypertrophy and reducing pain sensitivity, both in the early stages of exercise, but I would argue predominantly having an effect on neurophysiology. Furthermore, it is understood that a reduction in pain can occur at both the exercising limb and at distant sites suggesting there are local and systemic effects (Lemley, Hunter, & Bement, 2015).
Lemley, Hunter & Bement., (2015) have recently discussed the mechanism of conditioned pain modulation (CPM) influencing EIH. CPM is the term given to the inhibition of pain from a noxious stimulus when a second noxious stimulus is applied (pain inhibits pain). Therefore, if EIH has a systemic affect and it is linked with CPM perhaps performing bouts of exercise in a distal area from the injury site may facilitate an attenuation in pain perceived at the injury site.
Several authors (Bement & Sluka, 2016; Koltyn, Brellenthin, Cook, Sehgal, & Hillard, 2014; Lemley et al., 2015; Lima, Abner, & Sluka, 2017; Naugle, Fillingim, & Iii, 2013) have published extensively in this area, discussing the complex neurophysiological changes that occur with pain and the effects that exercise has on CPM in experimental and clinical settings. Of course, we shouldn’t forget the subgroups (fibromyalgia, myofascial pain, chronic low back pain) that may not receive the descending inhibitory effects that occurs with exercise. This understandably can make it challenging for the person living with pain and for the pain clinician advocating exercise as part of a pain management program. In this case, both parties can feel frustrated due to pain’s agency on the implementation of therapeutic exercise. In addition, if pain is reported at the injury site, it is common that exercise programs are often reduced in the short-term or ceased due to lack of progress in the long term.
So, at this point (if you have come this far) I suspect you are probably wondering what has all this got to do with acid sensing ion channels (ASICs)?
A lovely paper by Sluka, Winter, & Wemmie, (2009)(Kathleen is a bit of legend in my book!) discusses the role that ASICs might have in acid-evoked pain. ASICs are activated by tissue injury and inflammation due to acidosis. It is further understood that ASICs might also have a critical role in nociception. Now, those of us that have an understanding of exercise physiology will be familiar with the anaerobic system and anaerobic glycolysis. Sluka et al., (2009) explain that exercise can cause local pH to decrease in muscle which is sufficient to activate ASICs thus leading to nociception.
So what?
Well, A question that always crops up for me is how long do individuals need to exercise before they receive the effects of EIH. That is undeniably, a huge question! We are all familiar with the ‘one size does not fit all’ approach and if pain is an emergent phenomenon then how can we predict what the trajectory is regarding recovery for people to live better with pain. The thing is we likely can’t predict this but there are active approaches we can implement to try to attenuate pain. I’ll mention here that of course all the other psychosocial stuff is important.
Through my own reading of EIH papers (Bement & Sluka, 2016; Daenen, Varkey, Kellmann, & Nijs, 2015; Koltyn et al., 2014; Lemley et al., 2015; Nijs, Kosek, Van Oosterwijck, & Meeus, 2012; Rio et al., 2016; Vaegter, Handberg, & Graven-Nielsen, 2014)it seems that aerobic exercise and isometric contractions have had the greatest attention. Aerobically based EIH is variable ranging from about 12-30 minutes. In some respects, I don’t always have 30 minutes and it may at times be impractical to ask a patient to exercise for this duration of time during a session.
Exercise and acid-sensing ion channels
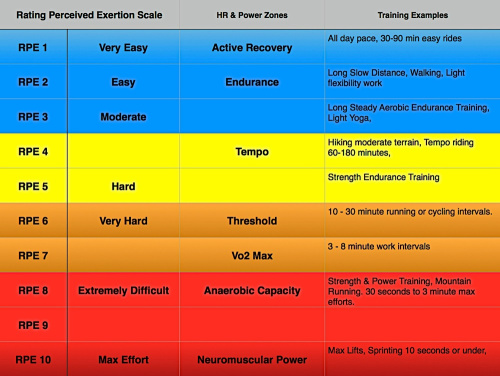
Perhaps we should explore the relationship exercise has with ASICs and CPM. As previously mentioned CPM is using a secondary noxious input to modulate a primary noxious stimulus. Through utilizing our anaerobic system we could potentially target ASICs to attenuate pain. Anaerobic glycolysis reaches its peak between 1.5 – 3 minutes (figure.1) (Katch, McArdle, & Katch, 2011). This is dependent on how trained the individual is and would mean discussing lactate thresholds, which is a whole other blog, so let’s not go there, today.

In individuals living with persistent pain perhaps it is possible to use short bouts of exercise in distal parts away from the affected area to promote EIH and facilitate an attenuation in pain (bear in mind the subgroups that don’t receive the phenomenon).
Let’s go through an example:
A patient is recovering from wrist pain following surgery. The physiotherapist prescribes exercise for the local tissue and due to repeated exercise (sets, reps etc) of the body part pain increases. A prolonged period of rest does not appear to reduce the irritability. So, by asking the patient to exercise a distal body part (let’s say body weighted squats down to below 90 degrees at the knee) rapidly at a high intensity for about 60 secs at an RPE of about 8 will promote anaerobic glycolysis (figure.2) and in theory stimulate local ASICs on chemoreceptors in the muscle tissue. Now, depending on thresholds and acid-base balance in the extracellular matrix of the neuron, nociception may occur if the squats are enough to stimulate this reaction. The theory would be that this would stimulate the CPM system resulting in a systemic effect and a concurrent modulation in pain at the recovering body part or wrist in this case.
It is certainly worth exploring and trying out with a select number of patients. It’s good to keep your curious hat on and think outside the box when it comes to working with people living with pain.
Respectively, the patient will benefit from this approach from a range of ways including becoming fitter, increase in confidence, promoting an internal locus of control, increasing independence and gaining self-management strategies. Remember it always makes sense to discuss and explore these options with your patient and ascertain their willingness to participate.
There are so many hacks that we can use with our patients to explore possibilities to address pain in our patients for more ways check out a previous blog post here.
Thanks again for having a read and as always, your comments are welcome.
TNP
References:
Bement, M. K. H., & Sluka, K. A. (2016). Exercise-induced analgesia: an evidence-based review. In Mechanisms and Management of Pain for the Physical Therapist, 2nd edn, ed.(2nd Editio, pp. 177–201). Seattle: IASP Press.
Daenen, L., Varkey, E., Kellmann, M., & Nijs, J. (2015). Exercise, not to Exercise or how to Exercise in Patients with Chronic Pain? Applying Science to Practice. The Clinical Journal of Pain, 31(2), 108–114. https://doi.org/10.1097/AJP.0000000000000099
Folland, J. P., & Williams, A. G. (2007). The adaptations to strength training: Morphological and neurological contributions to increased strength. Sports Medicine, 37(2), 145–168. https://doi.org/10.2165/00007256-200737020-00004
Katch, V. L., McArdle, W. D., & Katch, F. I. (2011). Training the Anaerobic and Aerobic Energy Systems. In Essentials of Exercise Physiology(4th Editio, pp. 409–442). Lippincott Williams & Wilkins.
Koltyn, K. F., Brellenthin, A. G., Cook, D. B., Sehgal, N., & Hillard, C. (2014). Mechanisms of exercise-induced hypoalgesia. Journal of Pain, 15(12), 1294–1304. https://doi.org/10.1016/j.jpain.2014.09.006
Lemley, K. J., Hunter, S. K., & Bement, M. K. H. (2015). Conditioned pain modulation predicts exercise-induced hypoalgesia in healthy adults. Medicine and Science in Sports and Exercise, 47(1), 176–184. https://doi.org/10.1249/MSS.0000000000000381
Lima, L. V., Abner, T. S. S., & Sluka, K. A. (2017). Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. Journal of Physiology,595(13), 4141–4150. https://doi.org/10.1113/JP273355
Naugle, K. M., Fillingim, R. B., & Iii, J. L. R. (2013). A meta-analytic review of the hypoalgesic effects of exercise. The Journal of Pain, 13(12), 1139–1150. https://doi.org/10.1016/j.jpain.2012.09.006.A
Nijs, J., Kosek, E., Van Oosterwijck, J., & Meeus, M. (2012). Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician, 15(3 Suppl), ES205-13. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22786458
Rio, E., van Ark, M., Docking, S., Moseley, G. L., Kidgell, D., Gaida, J. E., … Cook, J. (2016). Isometric Contractions Are More Analgesic Than Isotonic Contractions for Patellar Tendon Pain. Clinical Journal of Sport Medicine, 0(0), 1. https://doi.org/10.1097/JSM.0000000000000364
Sluka, K. A., Winter, O. C., & Wemmie, J. A. (2009). Acid-sensing ion channels: A new target for pain and CNS diseases. Current Opinion in Drug Discovery & Development,12(5), 693–704. Retrieved from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3494879&tool=pmcentrez&rendertype=abstract
Vaegter, H. B., Handberg, G., & Graven-Nielsen, T. (2014). Similarities between exercise-induced hypoalgesia and conditioned pain modulation in humans. Pain,155(1), 158–167. https://doi.org/10.1016/j.pain.2013.09.023

Hi,
May I ask who is the writer of this article?
Thanks
LikeLike
Hi Tashin,
I am
LikeLike