

Anyone who reads my blogs will know that I like to venture off the beaten track and explore how transferable knowledge between areas of interest or other specialties relate can be implemented into our understanding of persistent pain. I’ve blogged a few times about exercise dosage here, here and here and I thought I would add a further update to the series. I’ve been reading about overtraining syndrome (OTS) a bit recently and so for this blog I decided to 1) explore the comparisons between OTS and chronic pain (CP) and 2) using some of the models and terminology for OTS how we might transfer this knowledge into dosing appropriately for both groups.
Improving performance
To improve their performance or maintain their place in the team, �?athletes continuously work on their training regimen and dosage is an important part of periodization.
Simply, athletes share similarities with the general public. They strive for success, aim to fulfil their values, perhaps want to make some kind of contribution towards making a difference in the world, perhaps to inspire others. These things take focus and attention and naturally both groups are exposed to load.
When we talk about “load”, we should be acknowledging that it is more than just a weight or workload alone, as in a mechanical stressor. I am referring to load from a physiological, psychological, societal, cultural and mechanical perspective (Soligard et al., 2016).
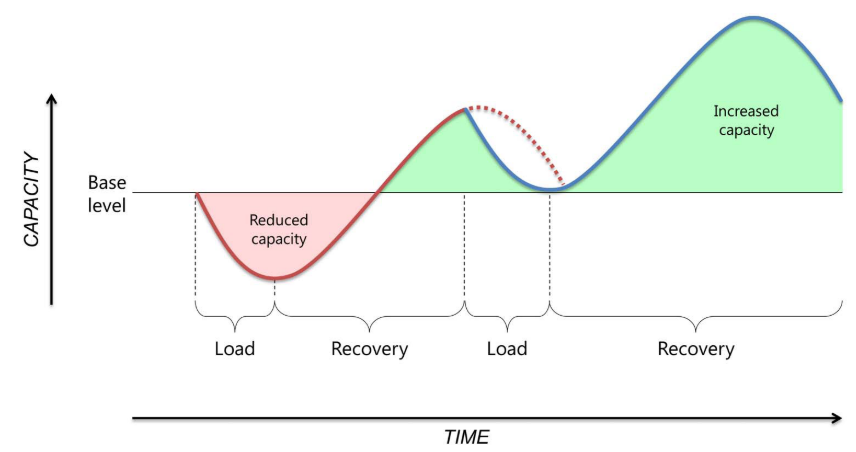
As athletes (amateur or elite) go through periodized stages of training throughout a season, they are likely to experience training barriers, be that physiological, psychological, societal etc. Successful training must be balanced involving overload and adequate recovery in order to gain performance increases (Figure 1). According to Meeusen et al., (2013) overload results in acute fatigue and following a couple of days recovery, results in an increase in performance. The principle of specific adaptation to imposed demands (SAID) basically means our body adapts and our tolerance and resilience increases. Whilst this principle is more commonly related to physiological change in tissue, we should consider the broader context of this principle to the human in society.
Considering the general public
Comparably, a member of the general public wanting to make gains in their career may feel that a strategy to improve their performance or climb the ladder is to increase their work hours or to read more journal articles (in my case!). This could be considered as an example of overload. As a consequence, following a period of adequate rest or reflection a positive improvement may occur, such as getting on top of work or updating sense making.
The point is we all start at a baseline and “load” our bodies and minds in a way that brings about adaptation. Think about when we start a new job or learn a language or a new skill. We go through highs and lows, some days are good, some… not so good.
Those same rules that apply to the athlete apply to the general public. The issue is when the acute stressor to gain the extra edge becomes an unhelpful habit where the underlying behavior is driven by a negative valence such as fear of missing out, or the person doesn’t feel they are good enough. As much of the research evidence appears to suggest, stronger predictors of disability are linked with psychosocial factors rather than physical factors in people living with long term pain (Chester, Jerosch-Herold, Lewis, & Shepstone, 2016; Costa, Maher, McAuley, Hancock, & Smeets, 2011; Menendez, Baker, & Oladeji, 2015; Piva, Fitzgerald, Wisniewski, & Delitto, 2009).
Overreaching and Overtraining syndrome
Back to athletes, the term ‘over-reaching’(OR) is related to a disruption in the balance between appropriate training stress and adequate recovery. The issue arises between determining if an athlete is in a state of OR or over-training (OT).
A definition for over-reaching
‘Overreaching: an accumulation of training and/ or non-training stress resulting in short-term decrement in performance capacity with or without related physiological and psychological signs and symptoms of maladaptation in which restoration of performance capacity may take from several days to several weeks’
Consider this term�? applied to a member of the general public:
‘Overreaching (perhaps overdoing might be a more appropriate word) – an accumulation of work and/or non-work related stress (think lifestyle, exercise levels, sleep, diet, relationships, thoughts, feelings, emotions) resulting in short-term decrement in physical or mental health (low mood, illness, fatigue, unhealthy habits) in which restoration of capacity may take from several days to several weeks.’
�?A definition for over-training
‘Overtraining: an accumulation of training and/ or non-training stress resulting in long-term decrement in performance capacity with or without related physiological and psychological signs and symptoms of maladaptation in which restoration of performance capacity may take several weeks or months.’
�?The same for overtraining in the general public:
‘Overtraining (perhaps rundown might be a more appropriate word) – an accumulation of work and/or non-work related stress (think lifestyle, exercise levels, sleep, diet, relationships, thoughts, feelings, emotions) resulting in long-term decrement in physical or mental health (low mood, illness, fatigue, unhealthy habits) in which restoration of capacity may take from several weeks to several months.’
There does appear to be some really strong comparisons we can make between athletes and the general public if we appreciate the broader context and perspectives of these definitions. An additional challenge is that injuries can occur due to the relationships between intrinsic and extrinsic factors.
The challenge is the nuance between the terms OR, OT and OTS (Table 1). As Meeusen et al., (2013) proposes there are many interacting factors that lead to OTS including biochemistry, hormones, inaccuracies in performance testing, psychological and physiological issues and the immune system. Similarly, we see much of these things involved in the chronic pain literature (O’Sullivan et al., 2018). So, like CP, OTS is not just the result of inadequate training load and recovery ratios.
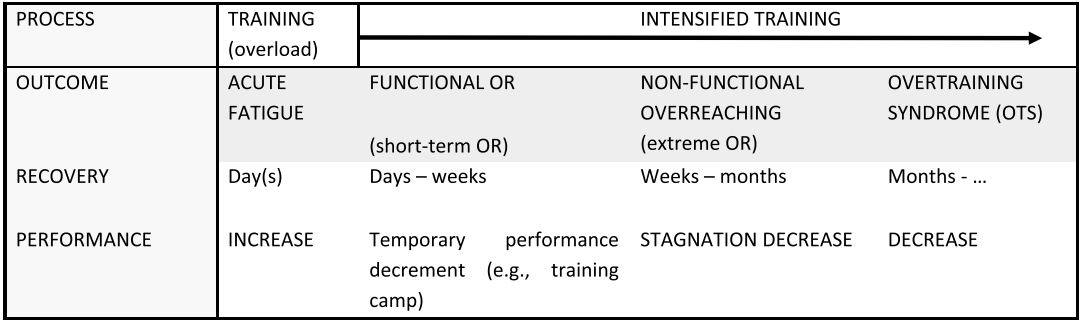
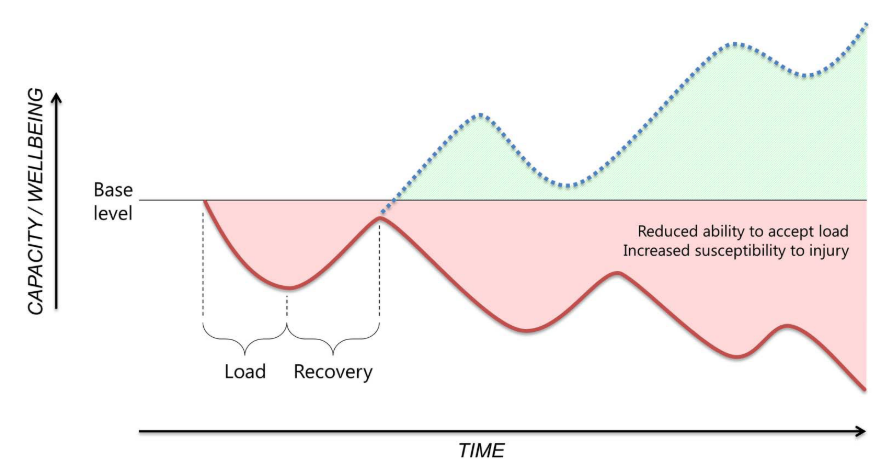
As shown in table 1, OR can be subcategorized into functional (FOR) and non-functional (NFOR). We can see that a prolonged period of over-reasching can lead to a steady decline in performance and the overall tolerance and health of the athlete.�? This is nicely depicted in Figure 2.
Supercompensation Segway
�?
What really caught my eye is the concept of ‘supercompensation’ effect in figure 1. Meeusen et al (2013) refers to ‘supercompensation’ as an effect following intensified training, resulting in performance decline followed by an enhanced performance after an appropriate period of recovery. The physiological responses of overreaching will compensate the training related stress. This really intrigued me because if we look at the literature around whether exercise should be painful in the management of chronic pain, Smith et al., (2017)proposes that improvements can be made in adults of musculoskeletal pain and protocols using exercises into pain have higher loads and doses of exercise.
Getting people going again?
All individuals (athletes and the general public) will have a baseline. Our initial and assessments help us to determine that baseline. The biopsychosocial considerations around OTS and CP should encourage clinicians to think of ways on how we can reduce load (biopsychosocial load) within sessions. Here’s a list of suggestions:
- Discuss flare ups in our initial sessions, why and how they happen, what they are, what they mean, and so educating people about them may mean that they are not as distressing when they do happen.
- Explore how self-efficacy strategies and goals can facilitate an increase in confidence and internal locus. This includes mastery experiences – recalling current and past achievements and savouring* those movements, observing others – seeing other individuals with similar CP complaints perform activities, therefore increasing willingness to try the activity, using verbal persuasions such as positive self talk and positive affirmations and thinking of our physiological/emotional states and using techniques such as deep breathing, attentional focus or mindfulness to reduce levels of distress.
- Use of measurement tools such as rate of perceived exertion (RPE) or Subjective Units of Distress Scale (SUDS) to provide clients with a way of externalising their distress and giving the clinician a subjective measure of feedback. This way exercise could be dosed accordingly within session.
- Setting goals that are meaningful and values based to the person, not for the clinician. For example, goals for the clinician are:
‘To improve range of movement with minimal symptoms’
or
‘To received pain education in order to improve coping skills’
These are NOT goals based on what is important and are of little value to the person.
Perhaps once we have accounted for psychosocial factors we can think of ways on how to dose exercise programs appropriately. In the case of supercompensation, is it possible that after a period of recovery from a flare up that we can dose the exercise program to be more directed to high intensity anaerobic training? More investigation needed!
Dosing Exercise – An update
�?An interesting meta-analysis by Polaski, Phelps, Kostek, Szucs, & Kolber, (2019) analyzed data from a comprehensive review (Geneen et al., 2017) specifically focusing on the dose of exercise intervention. Whilst they concluded the results provided insufficient evidence, they did propose the following:
‘While the present study cannot identify optimal values for dosing an exercise program or for�?detecting a significant pain effect between treatment and control groups for chronic pain,�?these results do suggest that varying exercise dose as measured by TIME, FREQUENCY and�?DURATION significantly influences a study’s measured effect size. And while changing “frequency per week” results in the most influential analgesic effect, this dose measurement is naturally limited to multiples of 7 days per week.’
�?There are two major conclusions I wish to make from reading the paper:
- The authors examined dosage as per the American College of Sports Medicine guidelines (Frequency = sessions per week, time = minutes of exercise performed in one week and intensity of exercise) and also considered duration as they wanted to evaluate the duration of study to allow for a novel examination of exercise effects. I am more interested at looking at dosage within session and how this then transfers into the week for the person living with pain. Whilst flare ups are regarded as normal, can we help to reduce the intensity of the flare or the duration with this approach?
- The majority of studies analyzed used a visual analogue scale (VAS) as measurement tool. Pain is multi-dimensional and subjective, so the VAS is just not a reliable tool for pain measurement. Perhaps the use of other subjective measurement tools such as rate of perceived exertion or subjective units of distress scale can be applied as a means of determining how a person is coping within session. Dosage can then be manipulated appropriately.
Encouragingly, studies as far back as 1996 have shown that using subjective measurement tools such as RPE to monitor training�?have demonstrated the utility of evaluating experimental alterations in training and have successfully related training load to its performance (Foster, 1998; Foster, Daines, Hector, Snyder, & Welsh, 1996). So, for those individual living with CP, could we be using RPE/SUDS more readily and confidently when dosing exercise? It is probable, but there is still a long way to go.
Summary
This blog intended to spark a few ideas regarding the comparisons between OTS and exercise in CP. In particular, the similarities between capacity, tolerance, recovery and resilience and how understanding the broader context of the individual person, beyond training loads (as in strengthening being primarily used to address pain), the clinician can use a variety of strategies and tools to consider how exercise could be dosed accordingly. An important point to consider is that this is not about finding a cure or fixing pain, this about facilitating relationships with the person, increasing motivation, seeing results and supporting the means for the person to engage in valued life activities.
Thanks for having a read.
TNP
*Savouring - Savoring just means that we attempt to fully feel, enjoy, and extend our�?positive experiences. Savoring is a great way to develop a long-lasting stream of positive thoughts and emotions, because positive events cannot always be relied on�?to make you happier.
References
Chester, R., Jerosch-Herold, C., Lewis, J., & Shepstone, L. (2016). Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: a multicentre longitudinal cohort study. British Journal of Sports Medicine, 0, 1–8. https://doi.org/10.1136/
Costa, L. D. C. M., Maher, C. G., McAuley, J. H., Hancock, M. J., & Smeets, R. J. E. M. (2011). Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. European Journal of Pain, 15(2), 213–219. https://doi.org/10.1016/j.ejpain.2010.06.014
Foster, C. (1998). Monitoring training in athletes with reference to overtraining syndrome. In Medicine and Science in Sports and Exercise. https://doi.org/10.1097/00005768-199807000-00023
Foster, C., Daines, E., Hector, L., Snyder, A. C., & Welsh, R. (1996). Athletic performance in relation to training load. Wisconsin Medical Journal.
Geneen, L. J., Andrew Moore, R., Clarke, C., Martin, D., Colvin, L. A., & Smith, B. H. (2017). Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews (Review). Cochrane Database of Systematic Reviews, (4). https://doi.org/10.1002/14651858.CD011279.pub3
Meeusen, R., Duclos, M., Foster, C., Fry, A., Gleeson, M., Nieman, D., … Urhausen, A. (2013). Prevention, diagnosis and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science (ECSS) and the American College of Sports Medicine (ACSM). European Journal of Sport Science, 13(1), 1–24. https://doi.org/10.1080/17461391.2012.730061
Menendez, M. E., Baker, D. K., & Oladeji, L. O. (2015). Psychological Distress Is Associated with Greater Perceived Disability and Pain in Patients Presenting to a Shoulder Clinic. Journal of Bone and Joint Surgery, 97(24), 1999–2003. https://doi.org/10.2106/JBJS.O.00387
O’Sullivan, P., Caneiro, J. P., O’Keeffe, M., Smith, A., Dankaerts, W., Fersum, K. V., & O’Sullivan, K. (2018). Cognitive Functional Therapy: An Integrated Behavioral Approach for the Targeted Management of Disabling Low Back Pain. Physical Therapy, 98(5), 408–423.
Piva, S. R., Fitzgerald, G. K., Wisniewski, S., & Delitto, A. (2009). Predictors of pain and function outcome after rehabilitation in patients with patellofemoral pain syndrome. Journal of Rehabilitation Medicine, 41(8), 604–612. https://doi.org/10.2340/16501977-0372
Polaski, A. M., Phelps, A. L., Kostek, M. C., Szucs, K. A., & Kolber, B. J. (2019). Exercise-induced hypoalgesia: A meta-analysis of exercise dosing for the treatment of chronic pain. PLoS ONE, 14(1), 1–29. https://doi.org/10.1371/journal.pone.021041
Smith, B., Hendrick, P., Smith, T., Bateman, M., Moffat, F., Rathleff, M., … Logan, P. (2017). Should exercises be painful in the management of chronic musculoskeletal pain? A systematic review and�?meta-analysis. British Journal of Sports Medicine .
Soligard, T., Schwellnus, M., Alonso, J. M., Bahr, R., Clarsen, B., Dijkstra, H. P., … Engebretsen, L. (2016). How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. British Journal of Sports Medicine, 50(17), 1030–1041. https://doi.org/10.1136/bjsports-2016-096581

Leave a Reply