
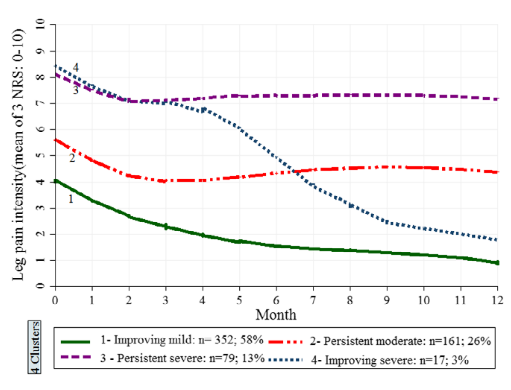
I’m not one for numbers and statistics and I’m not an academic, but I do like a graph that tells us a story. My attention was captured recently on twitter by a recent @tpmpodcast with @thomas_jesson discussing radicular pain, radiculopathy and sciatica (here). In particular was a graph that Tom posted on Twitter demonstrating the mean trajectory of 4 clusters of the course of low-back-related leg pain intensity over a 12 month period (see figure. 1).
Why did it capture your attention you might ask? Well, I believe it to be an important piece of information that clinicians could use to provide people living with pain a better understanding of 1) what may be contributing towards the persistence of their symptoms and 2) the fluctuating and episodic nature of pain. So I decided to take a closer look at a few studies, have a crack at examining clusters and trajectories and try to interpret the findings.
For 20 odd years, it has been recognized that Low Back Pain (LBP) is a multifactorial episodic condition and that if people have had LBP in the past it is likely they will have future episodes. In addition, there are varying degrees of severity reported over time courses that are categorized as chronic pain, but may be more or less disabling (Kongsted, Kent, Axen, Downie, & Dunn, 2016). Exploring the wider human experience of pain this may lead to stigmatization and perpetuate additional factors involved in the emergent pain experience (Cohen, Quintner, Buchanan, Nielsen, & Guy, 2011; Holloway, Sofaer-Bennett, & Walker, 2007). Therefore, this provides an argument against the simplistic categorical term of “chronic” which is classified as being longer than 3 months (Kongsted et al., 2016).
Trajectories and clusters
The first back pain trajectory study (according to the authors) was in 2006. Dunn, Jordan, & Croft, (2006)set out to demonstrate if they could identify and describe groups of primary care low back pain patients defined by changing pain patterns or stability of pain over time. So rather than classifying people as chronic the study identified that there are various classifications of chronic. Using longitudinal data they were able to classify back pain patients into distinct groups and track their pain over time. Collecting data from 342 patients and using a variety of statistical measures they were able to cluster 4 groups of back pain trajectories – Persistent mild, Recovering, Severe-chronic, Fluctuating. The clusters showed statistically significant differences in disability, psychological status and work absence, emphasizing the importance these factors have on the perpetuation and fluctuation of Chronic pain. The study also identified that pain and disability appeared to be correlated, that more pain means more disability.
Let’s skip forward 12 years and discuss the next paper. Acknowledging Dunn and Crofts earlier work, Ogollah, Konstantinou, Stynes, & Dunn, (2018)set out to determine trajectories of low-back-related leg pain in primary care patients over the course of 12 months (see figure 1). They wanted to specifically investigate prognostic factors thought to be associated with long-term outcome in low-back-related leg pain and in sciatica and also examine their independent effect.
Ogollah and colleagues used the data from a cohort of 609 patients from the Assessment and Treatment of Leg pain Associated with the Spine (ATLAS) trial (Konstantinou et al., 2012, 2018; Konstantinou, Dunn, Ogollah, Vogel, & Hay, 2015)and something called Growth Mixture Modeling (GMM) to identify clusters of patients with distinct leg pain trajectories.
Following assessment patients were managed according to one of three care pathways ‘(1) up to two physiotherapy sessions for those patients with improving or mild symptoms, (2) a course of physiotherapy treatment (three and more) for those patients with more troublesome pain, and (3) referral to secondary care; most patients in this pathway initially received a course of physiotherapy treatment’ (Konstantinou et al., 2018). Monthly data was collected over 12 months using postal questionnaires.
Referring to figure 1, you can see that all the trajectories, on average, over the first 3 months saw a decrease in leg pain intensity. 55% of the cohort reported improvement at 12 months, both in the sciatica and referred leg pain sub-groups. Ogollah and colleagues found longer leg pain duration, higher pain intensity, higher identity scores* and patient’s belief that the problem will last a long time were negatively correlated with improvement in disability. Meaning that this group of individuals were likely to be disabled for longer.
Interestingly, patients from the persistent severe and improving severe groups had higher scores of anxiety, depression, disability and sciatica bothersomeness than the improving mild and persistent moderate groups. So, what does this tell us? It would seem to support the evidence that back pain is episodic, variable, multi-factorial and that one size does not fit all.
Furthermore, the subsample with sciatica and corroborative MRI findings showed that “identity” remained independently associated with outcome. As I understand, this suggests that beliefs about symptoms were independent of findings on MRI. Therefore, those individuals with Sciatica type symptoms with corroborative MRI findings would have therapeutic options available to them such as surgery. I think it is useful to highlight that sciatica is often used as an umbrella term for leg symptoms. As such, distinguishing specific features that are associated with radiculopathy from radicular and somatic referred pain is an important part of the assessment procedure. If you would like to know more it is worth having a read of @thomas_jessons In Touch article here.
So what does all this tell us?
Well, not to get anyones hopes up, but evidence has identified that patients that are presented with trajectory illustrations can retrospectively identify themselves in named trajectory clusters and that this aligns with quantitatively-derived trajectories (Kongsted et al., 2016).
However, as I understand trajectories differ with respect to context (ah there’s that word again) and so placing people into clusters may mean we fall into the categorization trap again. I think this highlights that categorization does have a role to play but at the same time it is important to be aware of the uncertainty of how pain is episodic and can fluctuate in response to context. Clinicians can use trajectories to help normalize the episodic nature of pain.
I think trajectories kind of make sense, particularly if we think about pain. Much of the understanding of pain in society and the medical system is built upon the premise of the direct relationship between pain and pathology; in that if we address the pathology, pain will be “fixed” This is represented via the narrative and understanding that is placed upon interventional treatments such as manual therapy or radiofrequency neurotomy as unidimensional treatments for pain. As Ogollah and colleagues have identified these treatments as part of a multidisciplinary approach with an explanation of trajectory may change the outcome (Kongsted et al., 2016; Ogollah et al., 2018).
So, trajectories may be a useful prognostic tool to facilitate understanding of the episodic nature of (back) pain and also help to reduce misunderstandings around classifications of pain (acute, sub-acute and chronic). An example might be a flare up in an ongoing chronic problem being classified as “acute LBP”.
On the other hand do we risk perpetuating additional psychosocial factors such as anxiety or decrease capacity to cope due to a risk of normalizing pain as a trajectory and episodic throughout life. More research is required in this very interesting and important area of understanding pain.
Thanks for having a read and as always your feedback is appreciated.
TNP
*the sum of scores on seven symptoms – higher scores represent strongly held beliefs about number of symptoms attributed to the illness
Addendum
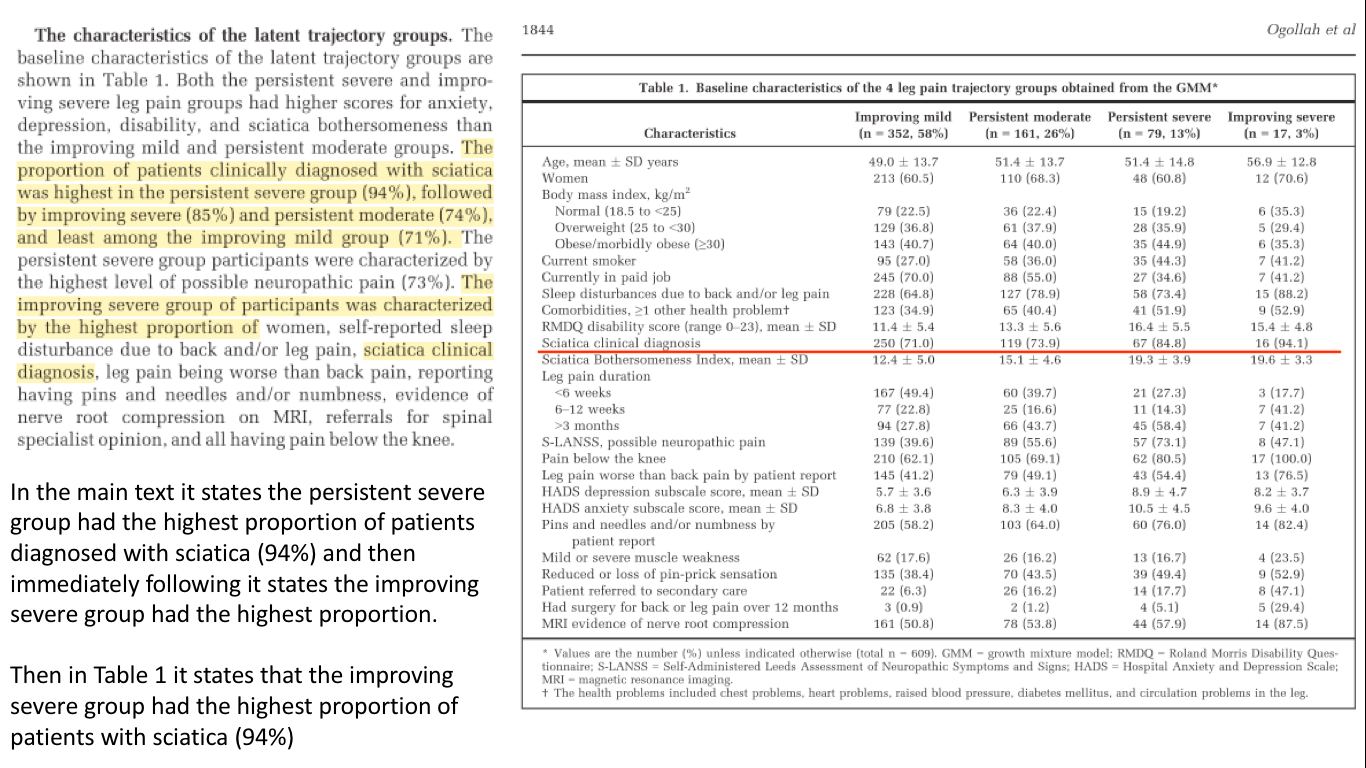
I forgot to add that there was an error in the Ogollah et al, (2018) paper. I suspect it was a type error as opposed to a data error and will likely not effect the results. See the image below
References
Cohen, M., Quintner, J., Buchanan, D., Nielsen, M., & Guy, L. (2011). Stigmatization of patients with chronic pain: The extinction of empathy. Pain Medicine, 12(11), 1637–1643. https://doi.org/10.1111/j.1526-4637.2011.01264.x
Dunn, K. M., Jordan, K., & Croft, P. R. (2006). Characterizing the course of low back pain: A latent class analysis. American Journal of Epidemiology, 163(8), 754–761. https://doi.org/10.1093/aje/kwj100
Holloway, I., Sofaer-Bennett, B., & Walker, J. (2007). The stigmatisation of people with chronic back pain. Disability and Rehabilitation, 29(18), 1456–1464. https://doi.org/10.1080/09638280601107260
Kongsted, A., Kent, P., Axen, I., Downie, A. S., & Dunn, K. M. (2016). What have we learned from ten years of trajectory research in low back pain? BMC Musculoskeletal Disorders,17(220), 1–11. https://doi.org/10.1186/s12891-016-1071-2
Konstantinou, K., Beardmore, R., Dunn, K. M., Lewis, M., Hider, S. L., Sanders, T., … Hay, E. M. (2012). Clinical course, characteristics and prognostic indicators in patients presenting with back and leg pain in primary care. the ATLAS study protocol. BMC Musculoskeletal Disorders, 13. https://doi.org/10.1186/1471-2474-13-4
Konstantinou, K., Dunn, K. M., Ogollah, R., Lewis, M., van der Windt, D., & Hay, E. M. (2018). Prognosis of sciatica and back-related leg pain in primary care: the ATLAS cohort. Spine Journal, 18(6), 1030–1040. https://doi.org/10.1016/j.spinee.2017.10.071
Konstantinou, K., Dunn, K. M., Ogollah, R., Vogel, S., & Hay, E. M. (2015). Characteristics of patients with low back and leg pain seeking treatment in primary care: Baseline results from the ATLAS cohort study Epidemiology of musculoskeletal disorders. BMC Musculoskeletal Disorders, 16(1). https://doi.org/10.1186/s12891-015-0787-8
Ogollah, R. O., Konstantinou, K., Stynes, S., & Dunn, K. M. (2018). Determining One-Year Trajectories of Low-Back–Related Leg Pain in Primary Care Patients: Growth Mixture Modeling of a Prospective Cohort Study. Arthritis Care and Research, 70(12), 1840–1848. https://doi.org/10.1002/acr.23556

Thank you for this.
In regards to the severe recovering pain group having higher scores on anxiety, depression…
In my own case, having RSD as well as DJD and sciatica…
First, as a severe pain flare improves if I don’t understand what triggered it in the first place I don’t know how to avoid it in the future and this inability to protect myself leads to anxiety. Secondly, pain is exhausting to cope with. As it improves there can be more energy to do other necessary and even fun things, but not knowing what I can safely do (see “First” above) leads to anxiety (catastrophic thinking, in my case). This increase energy with no good release ends up getting recycled into anxious behaviors and eventually depression if I’m not vigilant about this. Third, it has been extremely helpful to understand RSD correctly as a systemic disease. The hyperactive sympathetic nervous system can cause perpetual fight or flight type responses, which are not my typical responses when that system is kept in check.
LikeLike