
Hi all
It’s taken a bit longer than a week to get the second part up. Exams, courses, training, lecturer problems and a holiday took more of a priority.
So here’s part 2 of the Low Back Pain case study. Hope you find it interesting, perhaps of some value and of course I’m always open to feedback.
Assessment
As part of my assessment I use the electronic persistent pain outcomes collaboration (ePPOC) as a means to identify aspects of how the patient views their pain, the level of perceived disability, perceived distress, self-efficacy and how pain effects mood. The ePPOC includes the outcome measures the Brief Pain Inventory (BPI) Depression, Anxiety, Stress Scale (DASS-21) Pain Self-Efficacy Questionnaire (PSEQ) and Pain Catastrophising Scale (PCS) (Tardiff, Blanchard, Fenwick, Blissett, & Eagar, 2015).
As most of the outcome measures tend to determine the affective aspects of pain and how people view the reason for their pain, I also add in a questionnaire that aims to identify how pain affects activity levels. This may be a Pain Disability Index (PDI) or Patient Specific Functional Scale (PSFS).
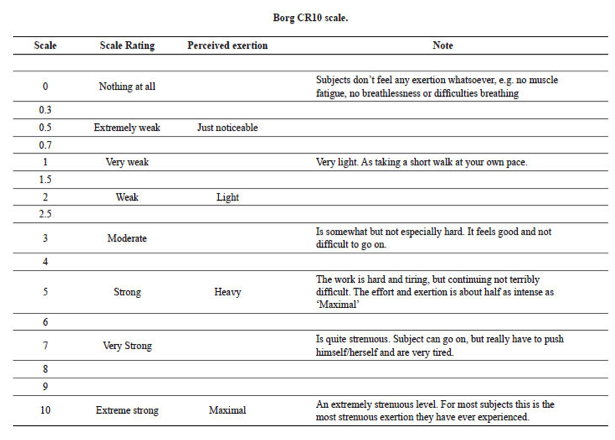
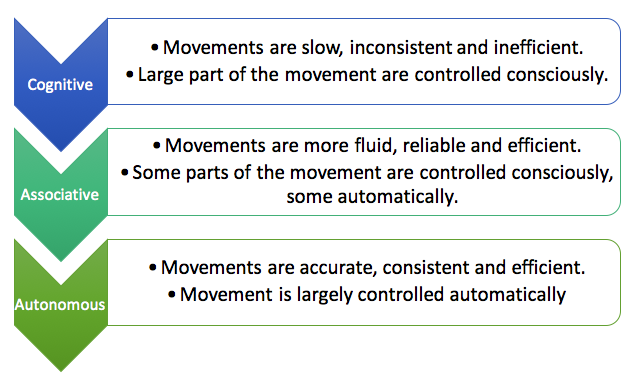
My approach is largely focussed on functional restoration through means of graded exposure based on the work of Vlaeyen et al, (2012). In order to provide a continual measurement of outcome I use subjective scoring methods such as rate of perceived exertion, discomfort, cognitive attention and harmfulness based on the Borg CR 10 scale (2010) (figure 2), Fitts and Posners (1967) 3-stage model of learning development (figure 3) and the Photograph of Daily Activities (PHODA) respectively (Leeuw, Goossens, van Breukelen, Boersma, & Vlaeyen, 2007). I have adapted PHODA that aims to identify (with the help of the patient) movements that are pertinent to her daily activities (bending and kneeling, lifting) and then measuring perceived harmfulness on a 1-5 scale (where 1 is too easy and 5 is too difficult). The images are adapted if achieved or too difficult and if not specific to work tasks (figure 4).

Intervention
My intervention would begin by carefully asking permission to discuss and challenge her beliefs about the structural and disease specific concerns that she has about her back. This would be based upon her history and also from clearance of sinister pathology (such as malignancy and fracture) which has a very low prevalence in persistent low back pain (1-4%) (Downie et al., 2013). Further discussion would aim to explain the prevalence of back pain in the adult population (Hoy et al., 2012) and also to provide an alternative explanation for her pain problem and associated activity limitations. As suggested by Vlaeyen et al., (2012) “mere reassurance that there is nothing wrong can have paradoxical and opposite effects.” (p. 1488)
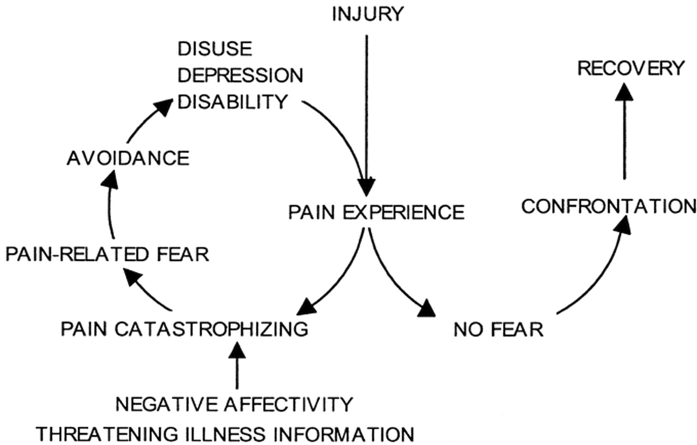
The patient identified difficulty with activities such as bending and kneeling during work and that she would sit down to perform activities rather than bending. Use of metaphor to explain the fear avoidance model (figure 5) (i.e. a reduction of fear of snakes by either flooding, which is likely to have repercussions, or a gradual introduction through pictures, videos, objects that resemble snakes, to real snakes) could provide a means of explaining what can maintain a pain problem, and also help to reframe beliefs and explore new methods for coping (Louw, Zimney, Puentedura, & Diener, 2016; Southall, 2013; M. A. Stewart, 2014; Vlaeyen et al., 2012).
Therefore, it would be appropriate to adapt the way the patient moved for a short time, this may include bending from the hips (if possible) and then to slowly introduce bending movements through the spine with decreased levels of threat, (lying on her back and drawing her knees to her chest), avoiding the perpetuation of fear, worry, stress or anxiety, and pain. Use of confrontation and expectancy violation approaches are ways of addressing the activity as a whole. If the patient had high levels of fear towards an activity (such as lifting a 3kg bag of shopping) due to it causing more damage to their back, it would be inappropriate to make the person perform this task. However, by adapting the activity in a way that would allow the patient to confront the problem in a less threatening way (bending to pick up a lighter object) is a means of violating a persons expectations towards the movement and activity. Any movements performed pertinent to activity would be scored using the subjective scales mentioned above, thus obtaining a perceived measure of ability. The movement is demonstrated prior to the patient performing the movement or activity, followed by a rescore of the subjective scales to obtain an actual measure of ability. This method would continue until a perceived reduction in fear was experienced and acknowledged. In addition, working towards a collaborative outcome of the patient challenging her beliefs, violating her expectations, and confronting her fears associated with movement (Craske, Treanor, Conway, Zbozinek, & Vervliet, 2014; Crombez, Eccleston, Damme, Vlaeyen, & Karoly, 2012; Leeuw et al., 2008; Vlaeyen et al., 2012).
Progression of activities would be advocated once improvements in self-efficacy and reductions in fear and worry were demonstrated. This might include a change in environment, minimising safety behaviours and promoting independence.
The aim would be to continue with progressions until the patient was able to reproduce the activities required with minimal disruption from beliefs, concerns or worry.
Confounds
Due to the number of scales and the time and effort it can take to rate activities or tasks there a number of confounds that may occur with this method:
- I am mindful that flare ups or relapses in pain levels can occur following treatment, often occurring the next day (I would highlight that flare ups are normal).
- Flare ups can occur due to other factors including changes in environment, poor sleep, societal influences, stress and safety behaviours.
- Flare ups may occur irrespective of the diligent use of the subjective scales.
- Encourage a slow and steady approach to minimise relapse or setbacks.
- I am mindful of the high levels of distress that can occur when asking patients to perform activities they may have anxiety towards.
Conclusion
As my work is primarily with people that live with persistent pain it is rare that psychosocial factors (particularly fear avoidance) do not present themselves. The video vignette demonstrates a common presentation of confounding factors that are prevalent in the population of patients that present to me in clinic. Therefore, the goal is to design a program that includes exposure activities that elicit the patients fear yet aims to have a favourable outcome towards confrontation.
So there you have it. I understand that many questions may come from this (which is the point!) and I realise that I could have discussed things with a lot more depth (word count restrictions).
Thanks for having a read
TNP
References:
Balagué, F., Mannion, A. F., Pellisé, F., & Cedraschi, C. (2012). Non-specific low back pain. The Lancet, 379(9814), 482–491. http://doi.org/10.1016/S0140-6736(11)60610-7
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., … Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American Journal Of Neuroradiology, 36(4). http://doi.org/10.3174/ajnr.A4173
Costa, L. D. C. M., Maher, C. G., McAuley, J. H., Hancock, M. J., & Smeets, R. J. E. M. (2011). Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. European Journal of Pain, 15(2), 213–219. http://doi.org/10.1016/j.ejpain.2010.06.014
Craske, M. G., Treanor, M., Conway, C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23.
Crombez, G., Eccleston, C., Damme, S. Van, Vlaeyen, J. W. S., & Karoly, P. (2012). The fear avoidance model of chronic pain: the next generation. Clin J Pain, 28, 475–483. http://doi.org/10.1097/AJP.0b013e3182385392
De Ruddere, L., Bosmans, M., Crombez, G., & Goubert, L. (2016). Patients are socially excluded when their pain has no medical explanation. The Journal of Pain, 17(9), 1028–1035. http://doi.org/10.1016/j.jpain.2016.06.005
Deyo, R. a, Jarvik, J. G., & Chou, R. (2014). Low back pain in primary care. Bmj, 349(July), 1–6. http://doi.org/10.1136/bmj.g4266
Deyo, R. a, Mirza, S. K., Turner, J. a, & Martin, B. I. (2009). Overtreating chronic back pain: time to back off? Journal of the American Board of Family Medicine : JABFM, 22(1), 62–68. http://doi.org/10.3122/jabfm.2009.01.080102
Downie, A., Williams, C. M., Henschke, N., Hancock, M. J., Ostelo, R. W. J. G., de Vet, H. C. W., … Maher, C. G. (2013). Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ (Clinical Research Ed.), 347(January), f7095. http://doi.org/10.1136/bmj.f7095
Eccleston, C., & Crombez, G. (2007). Worry and chronic pain : A misdirected problem solving model. Pain, 132(3), 233–236. http://doi.org/10.1016/j.pain.2007.09.014
Eriksen, T. E., Kerry, R., Mumford, S., Lie, S. A. N., & Anjum, R. L. (2013). At the borders of medical reasoning: aetiological and ontological challenges of medically unexplained symptoms. Philosophy, Ethics, and Humanities in Medicine : PEHM, 8(1), 11. http://doi.org/10.1186/1747-5341-8-11
Flynn, T. W. (2011). Appropriate Use of Diagnostic Imaging in Low Back Pain – A Reminder That Unnecessary Imaging May Do as Much Harm as Good. Journal of Orthopaedic and Sports Physical Therapy, 41(11), 838–846. http://doi.org/10.2519/jospt.2011.3618
Hoy, D., Bain, C., Williams, G., March, L., Brooks, P., Blyth, F., … Buchbinder, R. (2012). A systematic review of the global prevalence of low back pain. Arthritis and Rheumatism, 64(6), 2028–2037. http://doi.org/10.1002/art.34347
Karel, Y. H. J. M., Verkerk, K., Endenburg, S., Metselaar, S., & Verhagen, A. P. (2015). Effect of routine diagnostic imaging for patients with musculoskeletal disorders: A meta-analysis. European Journal of Internal Medicine, 26(8), 585–595. http://doi.org/10.1016/j.ejim.2015.06.018
Leeuw, M., Goossens, M. E. J. B., van Breukelen, G. J. P., Boersma, K., & Vlaeyen, J. W. S. (2007). Measuring Perceived Harmfulness of Physical Activities in Patients With Chronic Low Back Pain: The Photograph Series of Daily Activities-Short Electronic Version. Journal of Pain, 8(11), 840–849. http://doi.org/10.1016/j.jpain.2007.05.013
Leeuw, M., Goossens, M. E. J. B., van Breukelen, G. J. P., de Jong, J. R., Heuts, P. H. T. G., Smeets, R. J. E. M., … Vlaeyen, J. W. S. (2008). Exposure in vivo versus operant graded activity in chronic low back pain patients: Results of a randomized controlled trial. Pain, 138(1), 192–207. http://doi.org/10.1016/j.pain.2007.12.009
Louw, A., Zimney, K., Puentedura, E. J., & Diener, I. (2016). The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiotherapy Theory and Practice, 3985(August), 1–24. http://doi.org/10.1080/09593985.2016.1194646
Melzack, R. (2001). Pain and the neuromatrix in the brain. Journal of Dental Education, 65(12), 1378–1382.
Pitsoe, V., & Maila, M. (2013). Re-thinking Teacher Professional Development through Schön’s Reflective Practice and Situated Learning Lenses. Mediterranean Journal of Social Sciences, 4(3), 211–218. http://doi.org/10.5901/mjss.2013.v4n3p211
Ramond, A., Bouton, C., Richard, I., Roquelaure, Y., Baufreton, C., Legrand, E., & Huez, J. F. (2011). Psychosocial risk factors for chronic low back pain in primary care-a systematic review. Family Practice. http://doi.org/10.1093/fampra/cmq072
Southall, D. (2013). The patient’s use of metaphor within a palliative care setting: Theory, function and efficacy. A narrative literature review. Palliative Medicine, 27(4), 304–313. http://doi.org/10.1177/0269216312451948
Stewart, M. (2015). The assumption dilemma : do healthcare professionals have the teaching skills to meet the demands of therapeutic neuroscience education ?, 13(1), 40–42.
Stewart, M. A. (2014). The road to pain reconceptualization: Do metaphors help or hinder the journey? J Acupunct Assoc Chart Physiotherapists, (36). Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=amed&AN=0180670&site=ehost-live
Tardiff, H., Blanchard, M., Fenwick, N., Blissett, C., & Eagar, K. (2015). Electronic Persistent Pain Outcomes Collaboration National Report 2014. Australian Health Services Research Insitute, (University of Wollongong). Retrieved from https://www.noca.ie/wp-content/uploads/2015/11/IHFD-National-Report-2014-Online-Version.pdf
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., … Moradi-Lakeh, M. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2163–2196. http://doi.org/10.1016/S0140-6736(12)61729-2
Vlaeyen, J. W., Morley, S., Linton, S. J., Boersma, K., & de Jong, J. (2012). Essential guide to treatment. In J. W. Vlaeyen, S. Morley, S. J. Linton, K. Boersma & J. de Jong (Eds.), Pain-related Fear: Exposure-based treatment for chronic pain. Seattle: IASP Press.
