
As Paul flicked and gazed with interest through the latest journal article he became hot and flustered and pondered on how this new information could be disseminated and reasoned into his clinical practice. “I can’t stand it!” he cried as he thrust the journal to the floor in frustration. Yet, he became overwhelmed by the fiery heat building inside of him in reaction to the sensual urge to pick up the journal once again. He tore off his cashmere sweater with his masculine hands in protest. The feeling was too intense, he already had a university education and knew how to conduct a standard musculoskeletal assessment and yet his frustration intensified like a kettle, boiling, beginning to whistle as it reaches its peak of climax ready to blow its top. Paul slumped to the floor in defeat. Exhausted, he reached for the journal and succumbed to the tantalising content once more…
Ok, perhaps writing romantic novels is not for me, so I’ll stick with writing reflective blog posts instead. Strap yourself in this is a long one!
There is a point to that first paragraph. I do have a bit of a thing for critical and creative thinking. The idea behind thinking critically is not to be critical per se such as being an arse. Here’s a definition that fits with my biases of critical thinking:
Critical thinking is that mode of thinking — about any subject, content, or problem — in which the thinker improves the quality of his or her thinking by skillfully analyzing, assessing, and reconstructing it. Critical thinking is self-directed, self-disciplined, self-monitored, and self-corrective thinking. It presupposes assent to rigorous standards of excellence and mindful command of their use. It entails effective communication and problem-solving abilities, as well as a commitment to overcome our native egocentrism and sociocentrism.
Just in case those of you want to know what egocentrism and sociocentrism are:
Egocentrism – the inability to differentiate between self and other or being an arse
Sociocentrism – oriented toward or focused on one’s own special group or if you are an arse you’ll likely be drawn to other arses.
So, critical thinking is about listening, communicating, thinking, reflecting, reasoning, observing, reading, reviewing, collaborating and engaging the patient in these processes. It’s about being flexible and adaptable to allow for situations or context to change. Once you have done that, you formulate (with the patient) an appropriate framework that is coherent and flexible to the changing circumstances of the patient (Linton & Nicholas, 2008).
Something that has stuck with me is a reflective question that I constantly ask myself during a rehab session:
Why is this person presenting in this way at this time? And what can be done to reduce distress and disability?
This is a crucial question and (when we critique it) attempting to answer it is complex because the answer is frequently changing because many things about the person changes. I don’t think I need to elaborate further on the philosophy of man for those reading this to understand what I am getting at. There are many factors that will influence the pain presentation and so it pays to think more broadly or see a bigger picture when working with people living with persistent pain.
I am comfortable to admit that some of our more traditional methods of reasoning may fall short of the mark when it comes to supporting people with persistent pain.
Now I say may, I am not saying they do. Having done some reading around this topic (and I will admit I am no expert) Coderre, Mandin, Harasym, & Fick, (2003) have identified three diagnostic reasoning processes for solving clinical problems:
- Inductive reasoning - Follow a diagnostic process like an inductive tree. Is a logical process in which multiple premises, all believed true or found true most of the time, are combined to obtain a specific conclusion.
- Pattern recognition – the retrieval of an appropriate match based upon salient cues, when one case is similar to another
- Hypothetico-deductive reasoning (H-D) - clinician relates general knowledge of disease hypothesised to specific signs and symptoms of the patient. This method is often used when unable to use the other two reasoning processes commonly as a result of falling into a domain outside of expertise.
So, my take on these reasoning processes is that they are reductive and focus on the disease. They may also be unable to provide comprehensive links between diagnosis and causal relationships (Eriksen, Kerry, Mumford, Lie, & Anjum, 2013). Furthermore, Simpkin & Schwartzstein, (2016) argue that ‘the medical profession continually has to make decisions on the basis of imperfect data and limited knowledge, which leads to diagnostic uncertainty, coupled with the uncertainty that arises from unpredictable patient responses to treatment and from health care outcomes that are far from binary.’
Just to highlight again this is not to say that they are not useful. In acute medicine for example is where these reasoning process are necessary for clinicians. Having to make life or death decisions in an A&E doctors case or if a physio needs to make a call about an injury on the playing field. These reasoning processes tend to fall short when it comes to working with more complex problems such as persistent pain.
Interestingly, Loftus, (2011) contends that Fordyce’s (1976) onion skin model is hierarchical in nature, highlighting that the deeper layers are more foundational and therefore more important than the outer layers. Neurobiology is located at the base and the social world, the environment, at the periphery. As such more biomedically orientated students will consider the disease of the tissue as important as opposed to students that focus more on the integration of the person back into society such as occupational therapists and social workers.
Loftus, (2011) argues that medicines view of the ‘BODY AS MACHINE’ causes a handing over of ownership of our bodies to the medical or health professional to treat the disease.
‘Health professionals who focus on fixing the damage/disease but ignore the ‘worried, help-seeking persons’ do so at their peril.’
As such, the continued focus on BODY AS MACHINE has contributed to back pain being the most common problem associated with years lived with disability (Vos et al., 2012; Nicholls, 2016).
So, if these methods of reasoning fall short of the mark then what is the answer? Vertue & Haig, (2008) argue that an abductive reasoning approach that combines the diagnostic processes of clinical reasoning with case formulation, provides a flexible and adaptable framework that attempts to establish causal relationships to described and explained problems as presented in real time by the patient.
What is case formulation and how is it different from what we are doing already? Why does it fit better to understanding why a person presents to you the way they do better than the other processes? These are two questions I will attempt to answer.
What is case formulation?
According to Linton & Nicholas, (2008) case formulation involves:
- Identifying problem areas and factors that seem to be maintaining the problem
- Integrating information into a coherent framework, collaborating and goal setting with the patient
- Provides flexibility and adaptability in the management plan and provides feedback on whether goals are being achieved
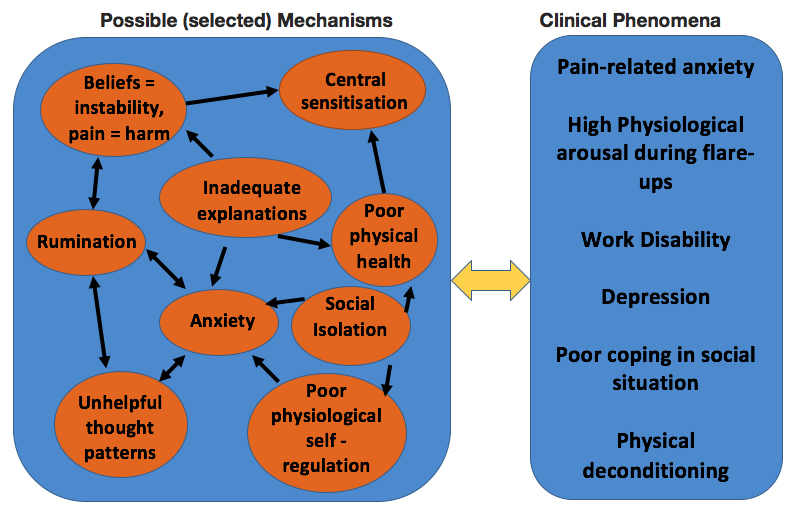
Vertue and Haig, (2008) provide a (5 phase) breakdown of the process of abductive reasoning to formulate a case. I have attempted to summarise and provide reflective questioning from a BPS perspective. I have also added a final schematic of the 5 phases identifying the intra and interdependence between possible mechanisms and clinical phenomena.
- Phenomena Detection – this phase involves data collection including why the person is seeking help and their level of function over a number of domains - think biopsychosocial or yellow flags. What salient cues are there that might make you consider that a social worker or a psychologist might be required? i.e. alcohol abuse, financial strain, emotional difficulty.
- Inferring Causal Mechanisms - this phase involves identifying plausible causal factors and linking empirical data to the patient’s clinical presentation. Remember the reflective question “why is this person presenting in this way at this time?” If we consider a biopsychosocial approach we should be looking at tissue trauma and associated risk factors – red flags etc. However more importantly how does the trauma affect the person? Do they believe that a “popping” sound in the back is a fracture? What evidence is there to support or refute this? The further question then is why? What vulnerability, fears or beliefs need to be extinguished in this case? What evidence is there to support or refute this? Do they have any habits i.e. avoidance of movement? What evidence is there to support or refute this?
- Developing a Causal Model - the next phase is to establish relationships between the mechanisms in a causal model – linking biopsychosocial mechanisms with clinical phenomena (see model below as an example)
- Evaluating the Causal Model – this phase evaluates the proposed model by examining the interrelationships between biopsychosocial mechanisms and clinical phenomena thus providing a coherent way to conceptualise why the person is presenting in this way at this time?
- Formulating the case – The final phase is the narrative of having brought everything together in a descriptive and explanatory way in an attempt to answer the question “why is this person presenting in this way at this time?”
Why does it fit better?
From my reading and experiences an abductive reasoning approach fits better due to the flexibility and comprehensiveness of the resulting causal model. Some may argue that this is no different than H-D reasoning and I would not necessarily contest that. However, H-D reasoning is still based upon identifying a diagnosis (of disease) with a causal relationship, and in many cases of people living with pain a diagnosis is often difficult to ascertain as the empirical data is showing poor causal relationships between pathology and pain.
Clinical reasoning and case formulation is appropriate as it represents an N=1 case that highlights vulnerabilities and strengths in the person and aims to provide a comprehensive means of supporting a person to live well with pain.
So why the title fifty shades of grey you ask? Well humans don’t do well with grey, it’s not a clear right or wrong, black or white, this or that, ying or yang, and as a society we don’t accept grey because it is steeped in uncertainty. Simpkin & Schwartzstein, (2016) state, ‘Too often, healthcare focuses on transforming a patient’s grey-scale narrative into a black-and-white diagnosis that can be neatly categorized and labeled.’
I wanted to end with a quote that I recently heard on the BMJ Podcast:
“The quote from Hofmann is entirely appropriate. That the issue here that perhaps for the last few hundred years, as different societies and cultures, but collectively we’ve developed this deep faith for medical science. This deep love for medical science because it can produce such extraordinary progress for human kind. We have treatments and tests that can extend our lives and reduce suffering, and extraordinary advances in our short lifetimes, but there is no doubt this has made us a little too blind to the downsides of what healthcare does, the downsides to medical tests and treatments. I think we are living in a time when we are learning more and more about the inevitable downsides of what we are doing. One of those things is that we have just been too enthusiastic for medicine and too enthusiastic to embrace diagnostic labels. Part of it is that in a sense, medicine holds out the promise of eliminating suffering, eliminating decay, eliminating disease, of eliminating death and this of course is an absurd dream, and it’s not really a dream it’s a nightmare because it’s leading us to test and leading us to diagnose and to treat way beyond what we need to do”
“An acceptance of the reality of human suffering could well help us deal with this problem of too much medicine.”
Thanks for having a read
TNP
References:
Coderre, S., Mandin, H., Harasym, P. H., & Fick, G. H. (2003). Diagnostic reasoning strategies and diagnostic success. Medical Education, 37(8), 695–703. https://doi.org/10.1046/j.1365-2923.2003.01577.x
Eriksen, T. E., Kerry, R., Mumford, S., Lie, S. A. N., & Anjum, R. L. (2013). At the borders of medical reasoning: aetiological and ontological challenges of medically unexplained symptoms. Philosophy, Ethics, and Humanities in Medicine : PEHM, 8(1), 11. https://doi.org/10.1186/1747-5341-8-11
Linton, S. J., & Nicholas, M. K. (2008). After assessment, then what? Integrating findings for successful case formulation and treatment tailoring. Clinical Pain Management Second Edition: Practice and Procedures, 4, 1095.
Loftus, S. (2011). Pain and its Metaphors: A Dialogical Approach. Journal of Medical Humanities, 32(3), 213–230. https://doi.org/10.1007/s10912-011-9139-3
Simpkin, A. L., & Schwartzstein, R. M. (2016). Tolerating Uncertainty — The Next Medical Revolution ? New England Journal of Medicine, 375(18), 1713–1715.
Vertue, F. M., & Haig, B. D. (2008). An Abductive Perspective on Clinical Reasoning and Case Formulation. Journal of Clinical Psychology, 64(9), 1046–1068. https://doi.org/10.1002/jclp
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., … Moradi-Lakeh, M. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2163–2196. https://doi.org/10.1016/S0140-6736(12)61729-2

Leave a Reply