

People in pain often describe how much their pain hurts, often displaying its level of intensity through facial expression and tone of voice. The word ‘intensity’ is defined as
‘the quality of being intense’
Another definition refers to intensity as:
‘extreme depth of feeling’
Quality refers to the words to describe the characteristics and feeling relates to the distressing experience. So, the word intensity is profound, it paints a picture that represents aversiveness, distress, fear, of which pain becomes self-isolating destroying word, world and self (George & Jung, 2015). A human’s yearning to feel and describe how we feel is key to our survival, but not necessarily the intensity of unbearable pain.
The ‘intensity of pain’ can often dominate the discussion between the physiotherapist and the person living with pain, inadvertently leading the physiotherapist down a rabbit hole of histo/anato-pathological differential diagnosis, resulting in a focus on tissue rather than the person.
The intensity of something can also have a profound effect on our memory. Just last month I completed a race in the beautiful Karangahake gorge. 21kms of running through bush! Amazing! I ended up pacing with another runner and, as you do, we got chatting. What was particularly interesting to me was how his first words (after a brief exchange of pleasantries) described that he was injured. Even more interesting was that he had recovered from his injury 3 years ago and he had lived with it for a duration of 5 years. Yet he referred to his injury and the intensity of the pain in the present tense. Despite all that he was running 21kms and completed it in just over 2 hours! Great stuff!
Duration Neglect
This got me thinking about a paper that I had read about something called duration neglect and the concept of peak-end theory.
Peak-end theory is a psychological rule in which an experience is evaluated and remembered based on the peak (most intense) point of the experience and/or the ending of the experience. Our recollection of events is impacted greatly by our interpretation of events experienced rather than the experience as a whole�?(Redelmeier & Kahneman, 1996).
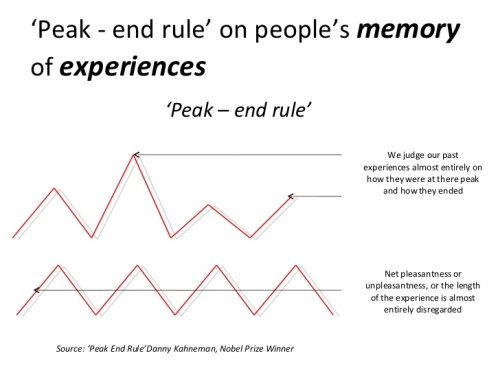
Peak-end theory was created by the Nobel Prize-winning Israeli psychologist Daniel Kahneman. His definition is as follows:
“The peak-end rule is a psychological heuristic in which people judge an experience largely based on how they felt at its peak (i.e. its most intense point) and at its end, rather than based on the total sum or average of every moment of the experience.”
Kahneman’s definition explains that cognitive biases affect our memories of our experiences and are generally dependent on the feelings we have during the experience. This is largely based on how we feel at peaks during the experience and at the end of the experience.
So, this suggests that irrespective of the duration of the experience this has little impact on the memory that is formed. Duration neglect proposes that the judgements people make on the unpleasantness of experiences is not attributed to the duration (Fredrickson & Kahneman, 1993).
The negativity bias
The notion of the negativity bias is associated with evolutionary biology (Ito & Cacioppo, 2005) and from that standpoint it makes sense that we would remember extreme experiences, positively or negatively. Establishing memories of negative experiences help us avoid similar situations in the future. Being able to recall positive experiences can help guide us to seek these situations out again.
In respect to pain, it is regarded as an aversive experience or negative experience. According to the negativity bias, negative attributes of an experience are often recalled more vividly than the positive ones. Therefore, cognitive biases towards pain experiences that are inherently negative or ‘intense’ may lead to an increase in fear avoidance and/or pain related anxiety.
Kahneman has investigated duration neglect within a pain setting. In one of Kahneman, Fredrickson, Schreiber, & Redelmeier, (1993) studies of duration neglect and peak-end theory in painful experiences, participants were subjected to two different versions of an unpleasant experience.
- The first trial had subjects submerge a hand in 14°C water for 60 seconds.
- The second trial had participants submerge the other hand in 14°C water for 60 seconds but kept their hand underwater for an additional 30 seconds, during which time the temperature raised by 1°C to 15°C.
Participants were then asked to select which trial they would most likely repeat. Interestingly, participants were more willing to re-do the second trial, even though they were exposed to uncomfortably cold temperatures for longer. Researchers concluded that participants chose the second, longer trial because they preferred the memory of it or disliked it less. In this study, it was supported that people judge experience how the event ends.
In another Kahneman study (Redelmeier, Katz, & Kahneman, 2003), participants underwent colonoscopy (this was at a time when colonoscopy was particularly unpleasant). One group had a standard procedure. The other group, after the procedure was completed, had the scope left inside, unmoving, for an additional 20 seconds. It seems, probes are not as unpleasant unmoving as they are when moving. The second group rated their experience with the colonoscopy slightly better than the first group. Kahneman and colleagues concluded the difference in the experience between the two groups was the second group experiencing a milder ending to the procedure.
In both studies the first group had an ‘intense’ unpleasant experience irrespective of the duration.
A reflection I have when I consider all the above is, “If we experience duration neglect, there must be a time when people living with pain don’t have pain that is intense as other times, and so how much is the negativity bias involved in duration neglect?”
(So What?) Before I provide an answer
If you have read some of my other blogs, you will see that I am bit of a rebel. I don’t just read evidence around physiotherapy because I believe that evidence should be about justifying strategies to help the population, not to solely justify the existence of a profession. I continue to experience a significant amount of tunnel vision and the Dunning-Kruger effect in the physiotherapy profession. Evidence-based practice seems to fuel dogma and it’s just a shitty combination for a profession with so much potential.
The point is reading other papers and applying that information into our practice is important. It’s innovative, creative and encourages serious playfulness.
To answer the so what question, consider the above phenomenon of duration neglect when working with people living with pain. Is there a way that you can make the experience of your sessions a bit more pleasant? Perhaps finish with a mindfulness session or a summary of achievements made in the session. Rather than the session being short and unpleasant, can you make it longer and give it a milder ending? Think about dosage (Frequency, Intensity, Time, Type) when doing an activity or setting a goal. Can you and the person you are working with come up with a strategy that they can use in their own time, when doing an activity that may be unpleasant? This rings all the hallmarks of ACT strategies such as defusion, acceptance and presence, all of which could come in very very useful.
Having a deeper understanding of pain and its broader psychological impact �?concurrently provides more opportunities to affect experiential avoidance, cognitive fusion or pain related fear or anxiety with the potential to affect pain intensity.
Thanks for having a read
TNP
References:
Fredrickson, B. L., & Kahneman, D. (1993). Duration Neglect in Retrospective Evaluations of Affective Episodes. Journal of Personality and Social Psychology, 65(1), 45–55. https://doi.org/10.1037/0022-3514.65.1.45
George, S. K., & Jung, P. G. (2015). Cultural Ontology of the Self in Pain(illustrate). Springer US.
Ito, T. A., & Cacioppo, J. T. (2005). Variations on a human universal: Individual differences in positivity offset and negativity bias. Cognition and Emotion, 19(1), 1–26. https://doi.org/10.1080/02699930441000120
Kahneman, D., Fredrickson, B. L., Schreiber, C. A., & Redelmeier, D. A. (1993). When More Pain Is Preferred to Less: Adding a Better End. Psychological Science, 4(6), 401–405. https://doi.org/10.1111/j.1467-9280.1993.tb00589.x
Redelmeier, D. A., & Kahneman, D. (1996). Patients’ memories of painful medical treatments: real-time and retrospective evaluations of two minimally invasive procedures. Pain,66, 3–8. https://doi.org/10.1109/PTC.2015.7232658
Redelmeier, D. A., Katz, J., & Kahneman, D. (2003). Memories of colonoscopy: A randomized trial. Pain,104(1–2), 187–194. https://doi.org/10.1016/S0304-3959(03)00003-4 LK - http://sfx.library.uu.nl/utrecht?sid=EMBASE&issn=03043959&id=doi:10.1016%2FS0304-3959%2803%2900003-4&atitle=Memories+of+colonoscopy%3A+A+randomized+trial&stitle=Pain&title=Pain&volume=104&issue=1-2&spage=187&epage=194&aulast=Redelmeier&aufirst=Donald+A.&auinit=D.A.&aufull=Redelmeier+D.A.&coden=PAIND&isbn=&pages=187-194&date=2003&auinit1=D&auinitm=A

Leave a Reply