

Over the last 2 days I have been plunged into one of many interesting debates on the twittersphere. I admit these days I prefer to be a bit more of a silent observer as I find your life can flash before your eyes when you become overly drawn in to social media conversations. In all honesty, I’d much rather be running and swimming.
The debate all started from a tweet from @honest_physio (see below) about the overuse of passive treatments for treatment. (One can only assume that these treatments were for pain relief). There was the usual toing and froing of request for papers to support people’s biases, which these days appears to have perpetuated dogma as opposed to try to dumb it down. Still, that’s just a separate observation.

I enjoyed the exchange of conversation, despite it lasting 2 days (and counting) it all appeared very civilized. Interestingly, was when the conversation turned towards exposure therapy and expectancy violation (in pain management).�? I’m certainly taken by this approach (yes it does support my biases) because it seems to fit nicely, like a finger in a doughnut ring, with the type of person I see in clinic. �?As we know though, not all fingers and doughnut rings are the same! (Strange how doughnut appear to have some kind of ubiquity in healthcare – the nocebo = doughtnuts for discs, the doughnut theory in tendinopathy)

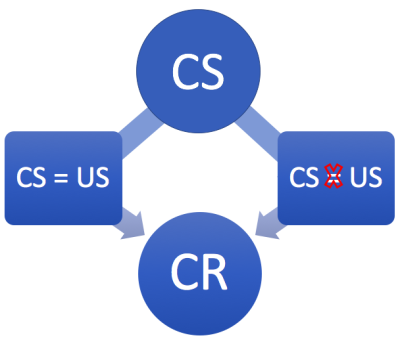
Back to exposure learning and expectancy violation.�?Exposure therapy was originally designed to treat phobias such as fear of spiders, heights, claustrophobia etc. The idea behind the concept was to attempt to extinguish the conditioned fear response (CR) from the pairing of a conditioned stimulus (CS) and an unconditioned stimulus (US)
The genesis of this pairing between CS and US is the basis for Pavlovian conditioning. Those of you that are familiar with Pavlovian conditioning will know of the famous experiment (which Pavlov stumbled upon whilst conducting another experiment) Pavlov’s dogs.
Michelle Craske is certainly an authority on exposure therapy/inhibitory learning and although her work is mainly to do with phobias, it is possible to extrapolate the information and apply within pain management. The fear avoidance model is well-known as a way to demonstrate the outcome of avoidance behavior perpetuated by the relationship between pain disability, affective distress and physical disuse. Johannes Vlaeyen, Steven Linton and others are the leading authority in this area (Vlaeyen & Linton, 2012). If you are interested it is worth reading some of their papers (Craske et al., 2008; Craske, Hermans, & Vervliet, 2018; Craske, Treanor, Conway, Zbozinek, & Vervliet, 2014; Den Hollander et al., 2016; Leeuw et al., 2008; Vlaeyen, De Jong, Geilen, Heuts, & Van Breukelen, 2001), but I warn you they are heavy reading!
What was nice to see in the exchange was a few blogs from Cory Blickenstaff (you can view them all here) regarding his understanding of them and how he implements them into his clinical practice. In particular, he posted his blog about symptom modification and his understanding of disconfirmation of beliefs. He explains how it can be challenging to disconfirm beliefs whether through education or symptom modification or other. The understanding being when we modify symptoms are we potentially promoting an adaptive or maladaptive change. For example, a maladaptive change MIGHT be “I’m not safe to move till I activate my core, which means that my spine is now strong”
The reason I say MIGHT is because in certain contexts the belief might be adaptive. Now, you might argue that the example I gave is never adaptive because we shouldn’t have to consciously think about activating our core. However, as we will see a bit later this may be beneficial to a person in a certain context.
I completely agree with Cory! After all (this is one of my favourite quotes ever) it was Bill Fordyce who said, “For behavior change, information is like wet noodles to a brick.” Essentially, Bill was saying that information alone is not enough for learning, experiential learning is an incredibly important part of understanding too. And as you will see later generalization is also incredibly important.�? To get a better understanding check out the clip here from the matrix.�?That entire film is a metaphor about learning, disconfirming beliefs, expectancy violation etc.
Cory, goes on to describe the use of expectancy violation to try to address the issue of “slippery” beliefs. You only need to go on social media and challenge someone’s beliefs (especially clinicians that are on there alllll the time!) to see how hard it can be to disconfirm them.
Expectancy violation is a way to address (maladaptive) beliefs. I’ll use Cory’s example. Let’s say the person with back pain has a belief that “hurt equals harm”, and that “bending forward leads to more damage in my back”. We can see that there are two components to this an action “bending forward” and a prediction “damage in my back”. At this point we could ask the patient to explain what they mean by providing a reflective account and asking an open- ended question. It might go something like this.
Person with back pain:When I bend forward it hurts so much, I’m concerned that I might do more damage to my back. The more pain I feel the more I’m concerned that I’m doing more damage.”
Practitioner:I can see that you are concerned about bending forward because, as I understand, this could lead to more damage of your back. �?Can you explain how that damage might affect you?
The responses might be varied – more pain, tightness in my back, unable to move. (You may even get a blank stare at the question!)
Cory continues in his blog by returning to the use of symptom modification as a form of expectancy violation. If you can modify symptoms in a way that gives the person internal locus (they discover change rather than the clinician changing pain for them), so that they CAN bend forward without confirming their expectations you refute the person’s prediction.�? I like to call this trickery. For example someone doesn’t like to bend forward in standing. So, I ask if they would be happy to sit down. More often than not they are happy to sit.�? I often ask people, “what position are you in now?” They look at me blankly and say tentatively, “uh, well sitting” I then ask, “if you did nothing else but straightened your knees, what position would you be in?” I often get a blank look and so I ask if I could demonstrate what that would look like.�? I then ask the patient “what position am I in?” The response is one of “bent forward.” At this point, this opens up a nice conversation about all the times we are bent forward and when their back is actually less painful. It also leads into conversations of tissue adaptation and tissue health.
Now, here’s a warning! I might scare people away from sitting after they have realized that they are bent forward! Thankfully, this has not happened.
So, I like using symptom modification but really only when it is actioned by the person and not by me. I am all about restoring internal locus and confidence and this can only be done when the person is in control. I believe I share that idea of symptom modification with many other clinicians.
I would like to add a bit more to this. We know from quite an extensive amount of research that disconfirming a paired CS and US is not really possible. In fact, it has been shown that once you disconfirm an association such as the back pain example above, it is very easy for it to resurface (Brown, LeBeau, Chat, & Craske, 2016; Volders, Meulders, De Peuter, Vervliet, & Vlaeyen, 2012). What appears to happen is that a new learning memory occurs. One that leads to the conditioned fear response and one that disconfirms it.
What to do about it? Well, this is where generalization and ACT come in very handy. This is not full proof remember. Different strokes for different folks!
So, what is generalization. Bill Fordyce understood that patients had variable lives outside of the clinic and so emphasized the importance of generalization (Fordyce, 2015). Quite simply generalization is about attempting to change the context as much as possible to further disconfirm the person’s expectations/predictions. This could take the form of a change in environment such as at home or work or in a park or on a beach, time of day, in quiet or busy places, varying sensory inputs like temperature or the speed of movement.
What this means is that we can’t just expect people to be all better once you disconfirm their beliefs by getting them bending in your physio clinic. You gotta get out of your place of selling sickness and change it up a bit!
It’s important to know that with this approach people will get distressed and using techniques from ACT whilst performing an exposure approach can be very helpful to modulate the affective aspect that can contribute to the person’s behavior.
Using ACT is a beautiful way of facilitating a shift in people’s focus away from struggling against their beliefs of what pain might mean to struggling less and considering what is meaningful and of value so that they see they can fly in the face of pain.
Thanks again for having a read of my musings.
TNP
References
Brown, L. A., LeBeau, R. T., Chat, K. Y., & Craske, M. G. (2016). Associative learning versus fear habituation as predictors of long-term extinction retention. Cognition and Emotion, 9931(April), 0–12. https://doi.org/10.1080/02699931.2016.1158695
Craske, M. G., Hermans, D., & Vervliet, B. (2018). State-of-the-art and future directions for extinction as a translational model for fear and anxiety. Philosophical Transactions of the Royal Society B: Biological Sciences, 373(1742). https://doi.org/10.1098/rstb.2017.0025
Craske, M. G., Kircanski, K., Zelikowsky, M., Mystkowski, J., Chowdhury, N., & Baker, A. (2008). Optimizing inhibitory learning during exposure therapy. Behaviour Research and Therapy. https://doi.org/10.1016/j.brat.2007.10.003
Craske, M. G., Treanor, M., Conway, C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23.
Den Hollander, M., Goossens, M., de Jong, J., Ruijgrok, J., Oosterhof, J., Onghena, P., … Vlaeyen, J. W. (2016). Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain, 0(0), 2318–2329. https://doi.org/10.1097/j.pain.0000000000000651
Fordyce, W. E. (2015). Fordyce’s Behavioural Methods for Chronic Pain and Illness. IASP Press. ISBN 978-1-4963-2029-2
Leeuw, M., Goossens, M. E. J. B., van Breukelen, G. J. P., de Jong, J. R., Heuts, P. H. T. G., Smeets, R. J. E. M., … Vlaeyen, J. W. S. (2008). Exposure in vivo versus operant graded activity in chronic low back pain patients: Results of a randomized controlled trial. Pain, 138(1), 192–207. https://doi.org/10.1016/j.pain.2007.12.009
Vlaeyen, J. W. S., De Jong, J., Geilen, M., Heuts, P. H. T. G., & Van Breukelen, G. (2001). Graded exposure in vivo in the treatment of pain-related fear: A replicated single-case experimental design in four patients with chronic low back pain. Behaviour Research and Therapy, 39(2), 151–166. https://doi.org/10.1016/S0005-7967(99)00174-6
Vlaeyen, J. W. S., & Linton, S. J. (2012). Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain, 153(6), 1144–1147. https://doi.org/10.1016/j.pain.2011.12.009
Volders, S., Meulders, A., De Peuter, S., Vervliet, B., & Vlaeyen, J. W. S. (2012). Safety behavior can hamper the extinction of fear of movement-related pain: An experimental investigation in healthy participants. Behaviour Research and Therapy, 50(11), 735–746. https://doi.org/10.1016/j.brat.2012.06.004

Leave a Reply