

We’ve all seen that familiar face pulled by people living with persistent who are being asked to exercise for the first time. Dosage is something we are all familiar with when it comes to taking medication. Yet with exercise will still tend to focus on the typical 3 sets of 10 or 12 or 15 often not considering how it affects the person living with persistent pain. Some, aren’t even keen to get into weights right away!
So what is the right dosage? How do we know when enough is enough or enough is too much? How should we be progressing people? Pacing is a very popular way of progressing people living with persistent pain, yet pacing has its limitations, frustrations and barriers to helping people with pain learn to live well. So, I want to share a few things that I use and do along with some of the evidence.
Another thing that I often hear is clinicians telling people to stop if there is pain when exercising. Nociception is the name given for the processing of noxious stimuli and as we know it is neither necessary nor sufficient for pain (Butler & Moseley, 2003).�? So, if we are working with someone with increased sensitivity then exercising with some pain may actually be ok.
A systematic review and meta-analysis last year from Smith et al., (2017) found that exercising with pain had benefits in the short-term but no real benefit from exercise of other treatment in the moderate and long term. On closer inspection of the selected papers it is important to note that participants were encouraged to exercise with the understanding that pain would not exceed 5/10 on a Visual Analogue Scale (VAS) and that symptoms would subside prior to the next bout of activity or the next day or before the next session.
As such Smith and colleagues identified that individuals exercising with pain provided favourable outcomes in the short-term. This is positive for us clinicians because we can feel reassured and reassure patients that it’s ok to exercise with pain. Remember it is important to note that pain is subjective and a 5/10 for one person during exercise maybe a 2/10 for another or an 8/10 for another doing the same exercise. Research is not representative of real world clinical situations but it can certainly help guide our reasoning to some extent.
Before I continue with dosage I think it is important to consider rest periods in between bouts of exercise. Nijs, Kosek, Van Oosterwijck, & Meeus, (2012) have provided some helpful guidelines for dysfunctional endogenous analgesia during exercise in individuals with persistent musculoskeletal pain. Personally, I monitor my patients constantly in terms of their recovery following a bout of activity or exercise. I use a variety of measures including time, heart rate (HR), Heart Rate Variability (HRV) and subjective scales including pain scales. One version of the Visual Analogue Scale I use is shown below.
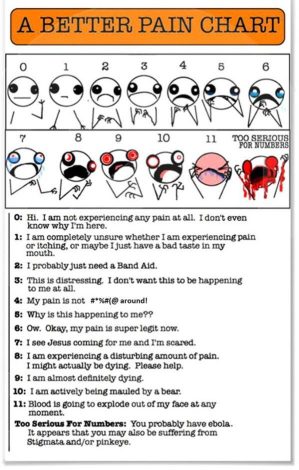
I use this scale to inject a bit of humour into the session because we all know laughter is the best medicine. Once the patient and I begin to see an improvement in their self-reported pain (which may take some time) I use pain scales less and less.
I also factor in that I’m not expecting people to be pain free. Most of the people I see present with multiple factors that we know can be potential triggers that perpetuate a pain state. I am very straight with my patients telling them that I am not looking for 100% pain free movement all of the time. �?If I get 20% out of 100% then that gives us a small window to show them that pain is not the same every time they repeat the same movement. This facilitates experiential learning and in time as the person sees the percentage of what they do increase patients self-reporting of pain reduces and the person becomes less avoidant towards pain.
I often use HR and HRV�?to monitor the patient’s reaction and recovery following exercise. As we all know pain is a multiple system output based upon perceived threat (Butler & Moseley, 2003). It is well documented that chronic pain can lead to dysregulation in the autonomic nervous system reflected in sympathetic and parasympathetic activity (Louw & Puentedura, 2013). Both can be recorded via HR and HRV (Tracy et al., 2016).

First, I should quickly define dosage. Dosage is made up of frequency (the number of times you exercise typically in a week), intensity (how hard you exercise) and duration (how long you exercise for recorded by time). In some cases, type (the type of exercise you perform – aerobic, weight training) and load (how much you lift) can also be considered. I think it’s also important to highlight that when I talk about load I’m only referring to weight in this context.�? Load can also represent the influence of multifactorial aspects affecting homeostasis. This is called allostasis and something I will touch on a bit later.
So, for an individual living with persistent pain who is beginning to exercise we should consider the dosage of exercise. Of course, I don’t need to remind you (but it looks…like…I…am?) that this should be based upon a collaborative understanding between patient and clinician.
Now, based upon an individual’s subjective history including psychosocial factors, psychometric scores and discussion of values, the individual can help me identify what may be more suitable for them in the immediate sense.�? This may be education or use of graded exposure or perhaps mindfulness. Some people just want to get going once you have given them permission to exercise! Admittedly, I tend to find that as people progress through their management plan there is often overlap between all the above. Through building a strong therapeutic alliance with the individual, together, we aim to promote internal locus of control and self-efficacy. As such, some individuals do progress onto more regular exercise.
Ok where was I? Dosage, right…so the beauty of using dosage is that you have many variables you can play with to find that sweet spot for that person. In the beginning, I would respect the individual’s experience of pain a bit more and as pain becomes less of a problem for them then I can play with the variables. The beauty of recording the data and placing onto an excel spreadsheet you can present a simple progress chart to the person to see how they are progressing.
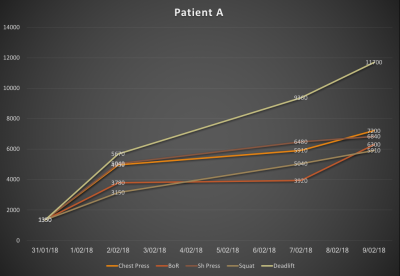
As nicely highlighted in Adam Meakins blog here by recording volume and increasing or decreasing variables you can keep a record of work done. Depending on how the individual works may have a positive or negative effect on volume.�? One example might be if the aim is for the individual to exercise for 2 sessions a week at 10 minutes on an exercise bike at a resistance of 4 resulting in an RPE of 6 the total volume would be 480. However, this may be unsustainable and let’s say they only manage 2 x 5 mins x resistance 4 x RPE 6 the total volume would be 240. Rather than using that information as a guide for the next session you could play with the variables. By breaking up the exercise into sub-variables such as breaking up the 10 minutes into 2 minute periods you could reach the same volume. So, 2 sessions a week x 5 bouts of 2 minutes at resistance 4 x RPE 6 = 480. Breaking up the 10 minutes and giving rest periods in between each bout is likely to encourage more adherence to exercise, and hopefully less disruption from their pain.
I have also found that as people introduce new variables, activities, movements to their life they often report flare ups. This often raises their anxiety in case they have done something bad. A good bout of reassurance and reflection on how far they have come since the start of the program often quells those concerns.
On a final note, I mentioned HRV earlier. I am using this more with my patients. HRV is the beat to beat variability in the heart rate time series.
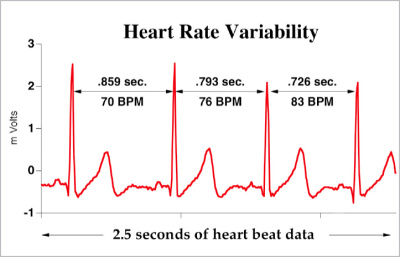
Heart Rate is under tonic inhibitory control by the parasympathetic branch of the Autonomic Nervous System (ANS). Sympathetic and parasympathetic nuclei receive input from descending inhibitory pathways (DIPs) involved in conditioned pain modulation (CPM). A systematic review and meta-analysis by Lewis, Rice, & McNair, (2012) identified that CPM is impaired in individuals living with chronic pain. Therefore, if descending inhibitory pathways are involved in CPM and CPM is impaired in individuals with chronic pain what impact does that have on parasympathetic activity and how is that reflected through HRV?
Well, a study by Koenig, Loerbroks, Jarczok, Fisher, & Thayer, (2016) identified impaired vagal activity through monitoring a specific parameter of HRV in individuals with chronic pain. Root mean square of successive differences or RMSSD is considered a time domain–based index corresponding to parasympathetic regulation of the heart.
It is also worthy of note that HRV is used in extensively in elite sport as a feedback tool to monitor training loads and essentially over-training (Plews, Laursen, Kilding, & Buchheit, 2014; Plews, Laursen, Stanley, Kilding, & Buchheit, 2013). Plews et al, (2013) found that increased time periods at high-intensity suppress parasympathetic activity, whilst low intensity training preserves and increases it.
A final thought. How does this translate into dreaded pacing regimes? Perhaps through using HRV it may help to do away with the frequent sense of failure people experience when they are unable to adhere to the incremental graduation of activity? Knowing that training at a lower intensity help to improve variability levels on HRV and concurrently vagal activity it may also benefit the clinician in periodising appropriate dosages and attenuate flare ups in the individual living with long term pain.
Granted, daily monitoring is likely required for HRV. There is a paucity of HRV research in health but it is slowly growing. Having played with it and done a bit of reading around the science, with appropriate reasoning and suited to a willing individual at best it can facilitate an understanding of how concerns, fears and stress are expressed through our physiology. As�?clinicians we have visual data to give patients, and who doesn’t like a bit of data to show how things are progressing.
As always, thanks for having a read
TNP
References:
Butler, D. S., & Moseley, G. L. (2003). Explain Pain. NOIgroup publications, Adelaide, Australia.
Koenig, J., Loerbroks, A., Jarczok, M. N., Fisher, J. E., & Thayer, J. F. (2016). Chronic Pain and Heart Rate Variability in a Cross-Sectional Occupational Sample: Evidence for Impaired Vagal Control. Clinical Journal of Pain, 32(3). https://doi.org/10.1097/AJP.0000000000000242
Lewis, G. N., Rice, D. A., & McNair, P. J. (2012). Conditioned pain modulation in populations with chronic pain: A systematic review and meta-analysis. Journal of Pain, 13(10), 936–944. https://doi.org/10.1016/j.jpain.2012.07.005
Louw, A., & Puentedura, E. (2013). Therapeutic Neuroscience Education: Teaching Patients About Pain, A Guide for Clinicians. International Spine and Pain Institute. OPTP publishing.
Nijs, J., Kosek, E., Van Oosterwijck, J., & Meeus, M. (2012). Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician, 15(3 Suppl), ES205-13. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22786458
Plews, A. D. J., Laursen, P. B., Kilding, A. E., & Buchheit, M. (2014). Heart Rate Variability and Training Intensity Distribution in Elite Rowers. International Journal of Sports Physiology and Performance, 9(6).
Plews, D. J., Laursen, P. B., Stanley, J., Kilding, A. E., & Buchheit, M. (2013). Training Adaptation and Heart Rate Variability in Elite Endurance Athletes : Opening the Door to Effective Monitoring, 773–781. https://doi.org/10.1007/s40279-013-0071-8
Smith, B., Hendrick, P., Smith, T., Bateman, M., Moffat, F., Rathleff, M., … Logan, P. (2017). Should exercises be painful in the management of chronic musculoskeletal pain? A systematic review and�?meta-analysis. British Journal of Sports Medicine .
Tracy, L. M., Ioannou, L., Baker, K. S., Gibson, S. J., Georgiou-karistianis, N., & Giummarra, M. J. (2016). Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. Pain, 157(1).

Leave a Reply