
Complex Regional Pain Syndrome (CRPS) is a severely debilitating condition. It’s been ranked higher than pregnancy and amputation of a digit on the McGill Pain Index. Currently, there is no single treatment specifically for CRPS. Yet this is a common trend with all complex pain presentations. A multi-modal approach is required due to the complex nature of the condition.
This blog is not specifically about all treatments for CRPS. I will be primarily looking at popular conservative approaches, those that are common in the Allied Health Professions (AHPs). For a full overview see (O’Connell, Wand, Mcauley, Marston, & Moseley, 2013).
Probably the most popular approach implemented by AHPs is Graded Motor Imagery (GMI). It’s a popular intervention for CRPS carried out by many AHPs that work in pain rehabilitation. I use GMI (particularly hand laterality) but like all treatment approaches it is not suited to everyone. I think a big problem is that in the Allied Health Professions there are a number of components that stand out:
- GMI is popular and has been marketed really well so it’s a go to treatment
- CRPS is becoming more recognized and so there is an association of GMI with CRPS.
- There is some excellent research associated with the GMI approach
- It’s cheap, relatively safe and has shown positive results in research conditions

Those of you that are familiar with CRPS are probably aware of GMI, which includes, mental imagery, left/right discrimination and mirror therapy (G. L. Moseley, 2004; G. Lorimer Moseley, 2005, 2006; L. G. Moseley, Butler, Beames, & Giles, 2012).
Despite the number of papers supporting the use of GMI, systematic reviews (Bowering et al., 2013; Smart, Wand, & O’Connell, 2016), topical reviews (G. Lorimer Moseley, Gallace, & Spence, 2008) and prospective clinical audits (Johnson et al., 2012) have identified a mix of positive and negative outcomes in the short term versus the long term, and a lack of high quality evidence to support its use compared to conventional physiotherapy approaches.
This poses an issue for people living with complex regional pain syndrome that have been informed about GMI as it may not live up to expectations. It also poses an issue for clinicians as GMI may not meet their expectations in terms of clinical outcome.
A study by Johnson et al., (2012) aimed to reproduce the early studies conducted by Moseley in a “real world” setting. Unfortunately, there were several factors that effected the intended outcome to reproduce that of what Moseley reported in his papers. This included less contact time with clinicians (patients were seen daily in Moseley’s studies), contact in “real world” was once every 2-4 weeks, training every waking hour was not feasible, patient contact time and monitored hourly training was not possible, and finally to factor in that research participants gain a great deal of attention, and the treatment outcome is regarded as the upmost priority. I think this is a large implication for most research versus “real world” scenarios.
We also have to consider that some people just get better over time (Bean, Johnson, & Kydd, 2014) and so this raises the question of how much more effective is the treatment over the natural course of the disease.
Now, it seems I have mainly critcised the use of GMI, however I believe this is important as we should all be much wiser to the idea that one treatment does not fit all and we should be appropriately reasoning when GMI might actually not work. I give you a quick case study example:
A patient I am currently working with had been receiving hand therapy and GMI since her diagnosis of CRPS in December 2016. So she had been receiving GMI for about a 9-month period. She certainly reported positive results in terms of her finger sensitivity and mobility, however she was still reporting mechanical hyperalgesia to pin-prick on the wrist, mechanical allodynia to wrist movement and tactile allodynia to light brush stroke, on questioning she reported that she would always pull her sleeve up away from her wrist. The patient also admitted a sense of avoidance to the limb and movement.
Two-Point Discrimination (TPD) found a 10-15mm difference in affected limb to non-affected limb. TPD is an assessment procedure that can identify reduced tactile acuity in the affected limb or area. Pain intensity has been linked with a decrease in tactile acuity and once pain reduces tactile acuity improves again (Maihofner, Handwerker, Neundorfer, & Birklein, 2004; Pleger et al., 2005). Now we can argue that reductions in tactile acuity can result from cortical reorganization and so GMI would be suited to this.
So, we assessed laterality (vanilla and context hands) and she had high percentage scores and quick reaction over 3 attempts. We also assessed how she reacted in the mirror box, there was no reproduction of pain in the affected limb when watching the reflected image of her non-affected hand move into the positons that were painful. Attempting to perform copied movements with the affected hand whilst watching the reflection of the non-affected also found that her proprioceptive awareness was out of synch. Watching the reflected image of the non-affected hand moving into wrist flexion or extension and attempting to reproduce with affected limb the patient thought both hands were in the same position when in fact they were not and so a mis-match was apparent.
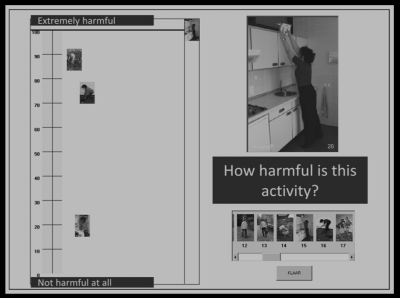
I decided to perform a Photograph of Daily Activities (PHODA) and adapted it to suit activities related to the wrist as that had presented with an aversion to her wrist and was also avoidant of pain. For info on PHODA see here. Her psychometric scoring also showed high levels of fear of movement (TSK), low self-efficacy (PSEQ) and high scores on the magnification subscale of the Pain Catastrophising Scale (PCS).
This was enough for me to reason that GMI probably would not have made much more of a difference. I felt exposure training to movement and context for the hand and wrist was more appropriate.
So, yes GMI has been shown to be effective (under research conditions) and has been adopted clinically, therefore it is important (when reasoned appropriately) to recognise other treatments that have been shown to deliver promising outcomes (under research conditions) that could be applied clinically.
Graded Exposure
Graded Exposure has been around for a long time. It was originally developed from work by behaviourists such as BF Skinner. Skinner worked with people that had developed phobias to neutral stimuli when they experienced a threat at the same time. Look back to my case study.
Vlaeyen & Linton, (2012) developed the fear avoidance model finding that a pain episode could lead to a perpetuating cycle of pain-related fear, avoidance behavior and disuse.
Studies identifying the use of Graded Exposure in CRPS (Den Hollander et al., 2016; Jong, Vlaeyen, Gelder, & Patijn, 2011) have shown promising results specifically in individuals that had signs pain-related fear. This would make sense if pain ‘is a multiple system output activated by the brain based upon perceived threat’ (Moseley, 2003).
After completing the PHODA we created a fear hierarchy of the selected activities and developed a graded exposure program. This meant that we would carry out activities not exactly the same as the activities on the PHODA but it did allow the patient to understand what we were attempting to achieve. At the same time during the activity I would ask the patient what she felt was happening in her body in response to the activity. This might include aversion, breath holds, rapid breathing, increase in heart rate, tensing. Think sympathetic nervous system fight or flight. The treatment will continue as per the graded exposure approach developed Vlaeyen and colleagues (Valeyen et al, 2012). I adopted this approach with many of my patients and it certainly is a challenging cognitive and reconceptualising experience for the patient.
So, to finish there are a number of important considerations:
- GMI is effective but only in certain conditions or circumstances
- That these approaches are not to be used in isolation.
- To not fall on the most obvious thing or most popular approach when you identify a condition. This is no different to applying manual therapy or acupuncture to every problem.
- That appropriate reasoning needs to be applied to every person that walks in to your clinic.
- That one may be viewed as a potential precursor to the next depending on findings from a subjective examination and the needs and expectations of the person in front of you.
- To know that you are not going to get it right every time and to not be afraid to ask for help – Man this is so important as a clinician. Whatever you think about feeling embarrassed that you don’t know what to do next is silly. What’s worse is carrying on and on with the person and they are not getting better.
Thanks for having a read
TNP
References
Bean, D. J., Johnson, M. H., & Kydd, R. R. (2014). The outcome of complex regional pain syndrome type 1: A systematic review. Journal of Pain, 15(7), 677–690. https://doi.org/10.1016/j.jpain.2014.01.500
Bowering, K. J., O’Connell, N. E., Tabor, A., Catley, M. J., Leake, H. B., Moseley, G. L., & Stanton, T. R. (2013). The effects of graded motor imagery and its components on chronic pain: a systematic review and meta-analysis. The Journal of Pain : Official Journal of the American Pain Society, 14(1), 3–13. https://doi.org/10.1016/j.jpain.2012.09.007
Den Hollander, M., Goossens, M., de Jong, J., Ruijgrok, J., Oosterhof, J., Onghena, P., … Vlaeyen, J. W. (2016). Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain, 0(0), 2318–2329. https://doi.org/10.1097/j.pain.0000000000000651
Johnson, S., Hall, J., Barnett, S., Draper, M., Derbyshire, G., Haynes, L., … Goebel, A. (2012). Using graded motor imagery for complex regional pain syndrome in clinical practice: Failure to improve pain. European Journal of Pain, 16(4), 550–561. https://doi.org/10.1002/j.1532-2149.2011.00064.x
Jong, J. R. De, Vlaeyen, J. W. S., Gelder, J. M. De, & Patijn, J. (2011). Pain-Related Fear, Perceived Harmfulness of Activities, and Functional Limitations in Complex Regional Pain Syndrome Type I. The Journal of Pain, 12(12), 1209–1218. https://doi.org/10.1016/j.jpain.2011.06.010
Maihofner, Handwerker, Neundorfer, & Birklein. (2004). Cortical reorganization during recovery from complex regional pain syndrome. Neurology, 63(4), 693–701. Retrieved from http://www.neurology.org/cgi/content/abstract/63/4/693%5Cnpapers://752201b3-22d6-48f6-a98b-954be6f25379/Paper/p199
Moseley, G. L. (2003). A pain neuromatrix approach to patients with chronic pain. Manual Therapy. https://doi.org/10.1016/S1356-689X(03)00051-1
Moseley, G. L. (2004). Graded motor imagery is effective for long-standing complex regional pain syndrome: A randomised controlled trial. Pain, 108(1–2), 192–198. https://doi.org/10.1016/j.pain.2004.01.006
Moseley, G. L. (2005). Is successful rehabilitation of complex regional pain syndrome due to sustained attention to the affected limb? A randomised clinical trial. Pain, 114(1–2), 54–61. https://doi.org/10.1016/j.pain.2004.11.024
Moseley, G. L. (2006). Graded motor imagery for pathologic pain: A randomized controlled trial. Neurology, 67(12), 2129–2134. https://doi.org/10.1212/01.wnl.0000249112.56935.32
Moseley, G. L., Gallace, A., & Spence, C. (2008). Is mirror therapy all it is cracked up to be? Current evidence and future directions. Pain. https://doi.org/10.1016/j.pain.2008.06.026
Moseley, L. G., Butler, D. S., Beames, T. B., & Giles, T. J. (2012). The Graded Imagery Handbook. Retrieved from http://books.google.com/books?hl=en&lr=&id=hh5lMD4DMakC&oi=fnd&pg=PP7&dq=graded+motor+imagery&ots=SKcSXWI_OK&sig=Hs8w32culWcE-9iuDaw2b-Sc_EY%5Cnpapers2://publication/uuid/FB7E5C78-5A23-40C1-B8D0-80848B8FF2C4
Pleger, B., Tegenthoff, M., Ragert, P., Förster, A. F., Dinese, H. R., Schwenkreis, P., … Maier, C. (2005). Sensorimotor returning in complex regional pain syndrome parallels pain reduction. Annals of Neurology. https://doi.org/10.1002/ana.20475
Smart, K. M., Wand, B. M., & O’Connell, N. E. (2016). Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database of Systematic Reviews, 2016(2). https://doi.org/10.1002/14651858.CD010853.pub2
Vlaeyen, J. W. S., & Linton, S. J. (2012). Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain, 153(6), 1144–1147. https://doi.org/10.1016/j.pain.2011.12.009

Grreat blog you have
LikeLike