Can we please stop pathologising! What does that mean? Well I am pointing the finger at you the clinician. This includes me! There are plenty of us out there who are guilty of pathologising and creating a society of hypervigilance.
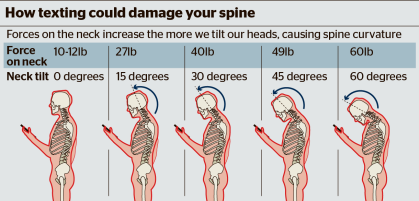
It’s a growing concern of mine that we continue to see trends of pathologising. I continue to see unhelpful information coming out about activities that we perform on a daily basis. A perfect example of this is the text neck nonsense.
I read that story and thought to myself how many times a day do I look down, so I decided to compile a short list.
- I look down when I go to get up from lying in bed
- I look down when I stand over the toilet to make sure I don’t miss the bowl
- I look down when I put my clothes on in the morning
- I look down when I’m making and eating my breakfast
- I look down when I put my shoes on
- I look down when I pat the dog or cat
- I look down when I’m treating my patients
- I look down when I’m reading a book, paper or journal
- I look down when I’m writing a blog post
- I look down when I’m vacuuming. cleaning, doing other household chores.
Ah but (I hear you all cry) the counter-argument is that the prolonged length of time that we are texting places extra strain on the neck. I would agree but that also highlights that it is not about texting it is about the prolonged time that we are looking down, the sedentary posture, but perhaps its more than just the mechanical effects, that healthcare professionals appear to be so transfixed on.
There are many other examples of overloading, what about the accountant that sits too much, builders that repeatedly lift too much, runners that run too much, rowers that row too much, hikers that hike too much? Hopefully you can see a picture unfold here regarding hypervigilance. What’s my advice for this? Well depending on your level of resilience, think about what you can do to avoid these prolonged activities. Break them up a bit throughout the day.
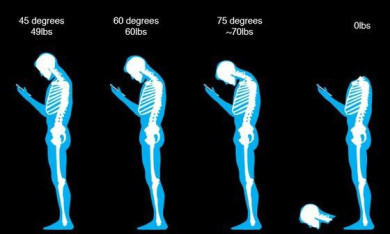
There are so many messages from clinicians, the media, social media and other mediums regarding what we should be careful of, and that there will be severe repercussions if we aren’t. We are becoming a hypervigilant society. We are surrounded by things that are consistently labelled as bad for us, such as the pictures of the text neck story that polluted our media and social media last year. Fortunately we were not fooled and very quickly an alternative picture surfaced.
More recently another picture has surfaced highlighting the orthopaedic perfect storm of sitting. This picture is directed at students and the younger generation. There are some classic words in there such as ‘douchebag’ shoulder and ‘kankles’ - way to go at affecting a kids self-esteem…..
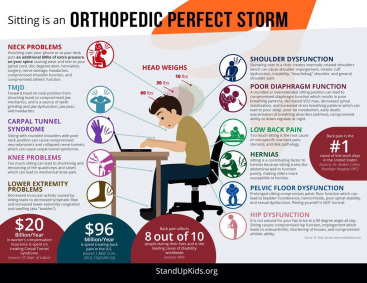
As if children aren’t stressed enough at school, learning different subjects, studying for exams, having to deal with bullying, going through puberty, pressure from peers and family to do well in all aspects of education and sport. Do we want to increase their stress more by telling them what could go wrong if they sit for too long? Sitting is just as bad for you as running would be if you didn’t rest. What next, are we going to start telling children not to participate in sport because of all the possible injuries they could be exposed to? What I find even more frustrating is that there are very few solutions to these so-called bad habits.
Why do we have to live in a society where everything is scrutinised as a bad habit. I recall having a conversation with a podiatrist about a seminar she had attended at a post-graduate lecture on incorrect lifting technique. You can read the article here. I don’t dispute that the forces are different between the two styles of lifting shown and that one causes less stress on the back. Yet does that really matter? If the task in front of the individual is perceived as a threat then it doesn’t matter how the item is lifted, the persistent back pain sufferer who has not lifted a box in years is unlikely to lift it.
A further example of poor communication and education I experienced recently was during an assessment of a hockey player. The player (now 20 years old) had a long history of shin pain (compartment syndrome) and last year had received his second bilateral fasciotomy of the posterior compartment*. The evidence for posterior decompression is weak and a recent paper has also highlighted a high level of interobserver variability in measurement of compartment pressures (reference, reference, reference).
Further questioning revealed that the player was informed that he lost around 50% of his calf muscle mass and he was told that he should not perform calf raises post surgically for 18 months. Paradoxically, he was told he could resume playing hockey after 8 months. Now either I’m really stupid or I’m completely missing something, but that just doesn’t make any sense to me. What this highlights is how we need to be so clear with our explanations and our education towards patients. The player continues to suffer with pain and his physiotherapy to date has now focussed on maintenance (acupuncture and massage).
I have highlighted before in a previous blog (here) that we have to be careful with our communication. There are many instances where we may think we are helping, but when our language, instructions, and advice are taken very literally it can result in mis-interpretation, and ultimately becomes a hindrance to recovery. As @jevnehelse recently posted up on twitter, we really do need to stop making our patients worse.
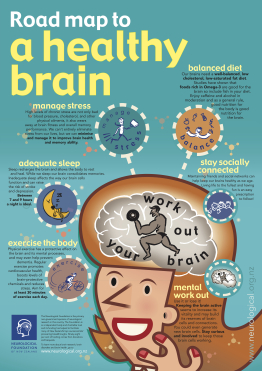
So how about some helpful posters…. The New Zealand Neurological Society have released a really helpful poster that encompasses several lifestyle aspects that support a healthy brain. If you maintain a healthy brain you reciprocally maintain a healthy body!
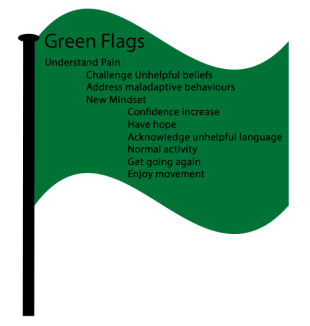
Louis Gifford was very much an evangelist in his clinical work and in writing his Topical Issues in Pain series of books. In that he wrote an excellent piece about pink flags. Louis explained that clinicians were very good at highlighting the bad such as pathology, yet not so good at informing people of how we heal and recover, unable to give timeframes. I feel that we are still very bad at this, somewhat hesitant of getting something wrong. So in order to help and for a bit of fun I have created green flags to facilitate our understanding of how we can wave the ‘green flag’ to encourage patients to get going again.
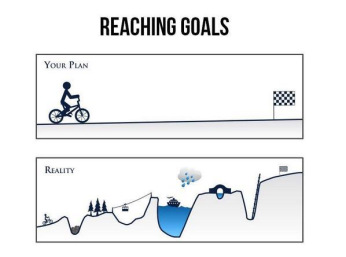
Clinicians require more support in being able to empower the public and our patients on the journey to recovery. It’s important that we are honest and realistic when educating our patients on this journey. Nothing is ever plain sailing, there will always be speed bumps along the way, but we can help by providing less of a focus on pathology and more of a focus on empowering patients to facilitate their journey to recovery.
So let’s start focussing more on empowering patients and being mindful of our communication. As all it takes is one mis-interpreted biomedical reference to create a snowball effect towards a cascade of chronicity (louw & Puentedura, 2013).
Thanks all for having a read and as always your comments are welcome.
TNP
* A common surgery for compartment syndrome is a fasciotomy or decompression, where it is understood that a surgical procedure releases the pressure in the leg resulting in an alleviation of pain.

Dear Sir,
Forgive me, as I am just a student phyio. But there is something that I don’t’ understand about this with regard to the ‘looking down’. This weekend I painted a ceiling, i spent the whole weekend looking up at the ceiling and that evening my neck was very very sore! I also work part time as a receptionist and after a few hours sat down at a desk staring at a computer screen, I ache everywhere. Equally, as we all do from time to time, i have spent to long looking down at my ipad ‘studying’ whilst sat on the sofa, and my neck aches after a few hours. All of these are reversible when getting up, moving around, stretching.
What I don’t understand regarding this pain science, and this article is that, it does cause pain when sat looking down for hours on end, as i think everyone has experienced at some point in their life. So what is the issue with telling people that it causes pain? Especially if getting up, moving around, stretching are all things that we should be doing anyway, not sat staring down at ipads.
I would appreciate any guidance with my confusion.
Many thanks
B.
LikeLike
Hi Bob
Thanks so much for your comment and what a great question!
I loved your comment about moving around and stretching to ease your symptoms and absolutely right it is what we should be doing. However the blog post was less about pain but more about the scare tactics and the fear that stories such as the text neck scandal create. Pathology and symptoms do not correlate. Pain is not a measure of the state of the tissues as we have discovered with countless MRI studies of patients with significant pathology but are completely asymptomatic. We cannot create a society of hyper vigilance (heightened concern) regarding pathology. A lot of serious pathology counts for a very small percentage of the population and you have to have other co-morbidities to be at risk of a red flag so the evidence tells us.
So you are absolutely right that holding your head in a single position for a long period of time is going to cause pain but that’s really important because its your brain and body telling you to get out of that position for a bit have a rest and then you can go back to it. I like to think of it as ‘use me but don’t abuse me’
We all naturally go through an ageing process so we are all exposed to the ‘kisses of time’. However we do not want to create fear avoidance by telling you that all these pathologies are made out to be more sinister than they actually are.
I hope that helps answer your question. Please do not hesitate to contact me again as I am always up for a good yarn about this fascinating subject.
Cheers
TNP
LikeLike
I don’t ‘mind’ the text neck poster. I had several older pts post Christmas with shoulder pain. Guess what they got for Christmas from their well meaning children? Tablets! They would sit on the couch and look down at them for who knows how long. I do agree that focusing on pathology or scare tactics isn’t what we should do - because for these people, it is simply changing the way they use the technology that would make the most difference - propping up the tablet and not holding it on the lap, etc. Being reminded to keep moving and alter position is very beneficial, but also recognising the perpetrator is important, just like Bob up there says - he knew his neck hurt from painting the ceiling. All that said - great article! 🙂
LikeLike
Thanks JM appreciate your comments, excellent points you make
LikeLike
Hi,
Thanks so much for you reply. So can I just clarify as if explaining it to a patient. The excessive “looking down/posture” etc is itself not a direct course of pathology? But the pain is an output from the Brain, as opposed to an input from the tissue? Is that correct?
Sorry for the garbled nature from my first question, sometimes trying to get thoughts to paper is hard, which is why I so appreciate the succinctness and easy to read nature of your posts!
Just as a follow up, why is the brain is telling you to move from these postures, if these postures don’t contribute to pathology directly?
Many thanks as always.
B
LikeLike
Hi Bob
Pain is 100% of the time produced by the brain. The receptors that live in your tissues are delivery systems (think of it like a postal service the delivery men are the nerves the sorting office is the brain) the final decision is down to the brain. However on the journey from tissue to brain the message can be amplified. (like a volume control the volume can be increased or reduced depending on the threat. Or I like to use Chinese whispers when you whisper in the next persons ear that Katie smells, the next person may make the whisper worse by saying Katie smells of rotten cabbages which may get a reaction of disgust in the next person or better by saying Katie smells of roses which should get a reaction of happiness. Continue the bad message and it can be perpetuated by using worse words and longer sentences or it could change altogether. I hope that made sense?) This can happen at the nerve in the peripheral nervous system, at the spinal cord level and even in the brain.
The excessive looking/down posture could be contributing to pathology yes but as we age we go through a natural aging process. (an example would be rotator cuff tears - 40% of 40 year olds, 50% of 50 year olds 60% of 60 year olds and so on have a form of rotator cuff tear, that may not be traumatic, this is acquired over time, so we are exposed to pathology throughout our lives) the issue is when the pathology is somehow correlated to symptoms and pain and is explained in a threatening way resulting in manual therapy or medication or injections and surgery is the only answer for example. (I apologise for the sweeping statement) It’s important to understand that we have been trained in a way that separates (dichotomy) our brain and our body. So when we have pain after lifting a box repeatedly and we see a pathology on an MRI then that must be the reason for the pain and symptoms. That is not the case.
If you are interested in learning more Bob can I suggest you have a flick through my web page or look up the work of Louis Gifford.
Please don’t apologise I appreciate your questions and I love to educate and be educated. So keep the questions coming! 🙂
LikeLike
The medical profession love pathologising. They love giving health issues a ‘medical term’. It helps them to neatly group things together and pop them in separate management boxes.
But there is a bigger reason and that is, the general public like having a special name for their problem.
So when B asks the question above “what wrong with telling them ?” I would say be careful what you say because their questioning usually has a deeper reason.
It’s the “…yes but what is ‘it’ called?” the “..what can I tell my boss/partner/husband/etc that it is?”.
This question usually comes after a clinician has spent ages explaining that the ‘it’ that they brought in to clinic was probably caused by, for example, sitting too much. That ‘it’ will most likely get better with some simple management change, a bit of time/patience. That ‘it’ needs very little treatment, possibly none and that “yes, of course your body can get things like this better !” reassurance
It’s then that the person will negate that what they caused with their ill thought through plan of for example, sitting for 12 hours at a desktop for three days, working on finishing their accounts, could just possibly have been the reason. That they just ‘over did’ sitting, combined with getting a bit stressed and now need to rest up and not spend another day doing the same.. This could gain the response “so you think it’s just that? I spent too long sitting at the desk?” “But what have I done? does it have a name?”
Its also the “well I looked up my symptoms on the internet and I wondered if it was iliotibial band syndrome, or runners knee, but then my friend said it might be a tendonitis…. I also wondered if it could be a recurrence of the osteochondritis I had 15 years ago?…”. People love pathology names.
So clinicians give names to problems because the public want a name for it. Then they can go away and look it up and read all about it and tell everyone that they have ‘it’
Here are some tips to design your own pathology. If something is inflamed add ‘itis’ to it. Here are some examples: Dermatitis, appendicitis, tonsillitis, tendonitis, myositis, chondritis
If it keeps coming back or doesn’t go away put the term “Chronic” or “Persistent” Some example are Chronic Fatigue, Persistent Pain
If there are lots of possible effects which could be grouped together call it a “Syndrome”.
Even better dress it up in latin. This makes it really cool because very few people will be able to translate it.
Then there are diseases. A disease can be defined as a particular abnormal condition, a disorder of structure or function, that affects part or all of an organism.
In which case “Sitting Disease” is a pretty cool one, because sitting too long has no beneficial effect. Its a completely unnatural thing for an animal to do. We need to spread the revolution and get people moving standing, carrying out natural movement and then maybe we can stop the pathology name game
LikeLike
Hi Jill
Thank you for your comment, very valid points made. What is very interesting are all the other factors behind pathologising. Sociological, philosophical, societal, environmental etc etc. It highlights the vast complexity of treating chronic diseases such as persistent pain, how it can be perpetuated, how it is individual to every single person on the planet, that you cannot group people together (well you could but everyone would still have a slightly different thought or behaviour).
I have no real answer as there are a gazillion reasons why an individual might experience pain. What I would say is exactly what you highlighted that these things can occur as we age (the kisses of time) and you can continue a normal life with them. It’s the scary language or patient blame game or egomaniac attitude that is used to create a society where we require something to fix it, when understanding that a lot of these things happen as we age and that (as you have also said) getting people moving, standing, carrying out normal natural movement we can stop playing the pathology name game. However if I wanted to play the pathologisng counter argument - what natural movement is to one person, could be causing harm in another………. the debate continues…..
LikeLike
“So clinicians give names to problems because the public want a name for it.”
I think it’s the other way around. We want names, cause our health care system triggered us to ask for them over years. We forgot, that we have a own responsibility for our body and mind - we forgot to stay in touch with both of them to keep healthy. And why?
We often hand over our responsibility to clinicians, because our society learned us to do so. We’ve learned that there are experts, who solves our problems and that we are “helpless people” who are not able to handle our problems. And we as clinicians treat them like that. We want them to do things, which they not (always) understand, we give them advice what they should (not) do, etc. We put us on a higher hierarchy level, take all the responsibilities from the client and make him/her helpless.
For me, communication skills are the key factors to solve that sort of problems. We have to start interacting with our clients on the same level. We have to give them their responsibilities back. Instead of telling the people whats “wrong” with them we should start asking the right questions, so they can “explore” their problems on their own. Instead of telling the people what they should to, we should start asking them which inner ressources they have/can use to solve their problems.
For me it’s not the public’s fault that they speak in pathologies, for me it’s the “healthcare’s” fault. If we, as clinicians want to improve something in the system, we have to ask ourselves, what we can do better and do it. Is it our taks to make our clients anxious by giving them pathologies, or is it our task to help people understand, why their problem has risen up and to coach them through the solving process until they are able to solve/handle it on their own?
LikeLike
Hi Georg
I’m not sure what else I can add to that, you make some very poignant points, excellent!
Thank you!
LikeLike
Hi! I love the article and the positive approch that empowers people instead of pathologizing them. What I miss a bit: Taking the example of “looking down” it seem as if there is only one choice: You can do it - but don´t stay to long in this position. But this gives that impression as if there is just one way of looking down!
But there are many different ways on “how to look down”, depending how much you involve your AO-joint, the hip joints etc. So it is possible to lock down for a long time without getting “stuck” if you see looking down not as a “position” but as an ongoing sublte movement. And it is FUN!!!
Waving to you with all my green flags from Bremen, Northern Germany
Stefanie
LikeLike
Thanks Stefanie, absolutely! It’s an interesting point you make. Contextually would it hurt as much if it was fun compared to if it wasn’t fun and you had to do it as part of a job that you hated and you were stressed because of the work piling up? 🙂
LikeLike
Well - I think it would hurt the same. But if it was fun we would probably say “It was worth it”. 🙂
Last weekend we painted with two people a 75 qm flat (twice 🙂 ) including the ceiling in two days. I am absolutely not used to this movement, I am small, not very strong and it is not my favorite way of fun… But when I decide to do it - or when I have no choice - I make myself as comfortable in my body as I possibly can. I make “doing this unloved work in the most effective, elegant, ergonomic way” my primary challenge. Afterwards I was exhausted, my muscles ached a bit, but no pain, stiff neck etc…. Everything fine after a warm bath and a good sleep…
The interesting thing I notice with my clients is: As soon as this process of “making selfcare my primary attidude” starts strange things happen: Sometimes the work goes easier, it becomes easier to say “NO”, you react earlier to stress, collegues are friendlier, the time management easier - or: If this does not happen - if the system you work in is built in a way that you have to sacrifice your coordination and health to it - people suddenly find the strength to speak up or find themselves a new job.
And this is not an easy, smooth process. This can be disturbing, frightening.. But when people listen to their bodies they get excellent feedback and motivation. I am always again surprised by this.
I am looking forward to your next blog posts. Stefanie
LikeLike
Well yess.. over over over and to much pathology.. but for those unfortunate people who have chronic issues and comorbidities.. they are left without aid to long so everything colapses. It will turn out allright isnt going to do it for them since a terrible chainreaction occurs leaving them below zero. For them i do recommend action at once, to prevent rapid decay and sometimes years to normalize. Without a latin word for it you don’t get the proper aid. So as i think surely not to overprotect and scare people .. people with chronic problems are often ignored out of this same idea and that wil just maje things worse for them. Life quality goes down drasticely and might take years to recover from.
LikeLike
Hi Elena
Thank you for your comment. This was one of the many reasons I wrote the blog is that for some non-specific musculoskeletal problems clinicians have and continue to cascade people into chronicity. Language, communication and education is a significant player in an individuals recovery. I know many a clinician specialised in understanding persistent pain that want to help those people that feel ignored. You are absolutely right in that saying it will turn our alright is completely inappropriate and unethical. The support networks are beginning to grow as more and more clinicians are being educated about understanding pain.
Thanks
LikeLike
Have you checked out https://www.painscience.com/articles/structuralism.php ? Very relevant to the “don’t pathologise idea.
LikeLiked by 1 person
Nope but I will do! Thanks for the link 🙂
LikeLike