
Hi all
I thought I would put a quick post in about my physiotalk I hosted on Monday the 2nd of March on professional boundaries. A topic that clearly affected all that participated in the chat with some really important issue raised. It was a busy hour generating a lot of discussion and 1 million impressions!
So I’ve decided I’ll go back to the beginning about how I got roped…..I mean asked to host a chat on professional boundaries. November last year I attended a 1-day Crossfit course in Christchurch. �?A fairly professional set up I met the instructor who was a Physical Therapist from the United States. I attended with my 2 other colleagues with the rest in attendance being personal trainers. The morning started off fairly well with a low down of what was to be expected, this abruptly came to a halt when I was concerned to hear that the physical therapist was going to teach us all how to diagnose, clinically reason and treat hip, knee, ankle and shoulder mobility problems (yes in relation to Crossfit). Did I mention that the course was a day course!!
As the day went on I became more concerned about the Physical Therapist educating trainers with no understanding of pathology, assessment, manual handling, clinical reasoning to name a few in a long list of concerns! So I decided to write a blog about it, you can read it here. So this sparked my small brain into gear regarding what our standing is on professional boundaries. I asked a few individuals on twitter and suggested a physiotalk was held on the very topic. The lovely girls at Physiotalk took no time at all to encourage me to host it.
What?…….me?………no……I couldn’t possibly…….plus I think I’m washing my hair that morning!!! Janet and Naomi were�?absolutely awesome and very helpful! So without further ado let’s get on with my run down of last Monday’s Physiotalk!
The morning began (or evening for everyone in the UK) with the first question�?‘What do we understand by professional boundaries?’�?After a slight issue with clarification the snowball developed (can I just add if you have ever used tweetdeck it is crazy!! If you plan to host a Physiotalk I suggest you practice and learn the ins and outs of its use not whilst on the job!)
Questions came in to clarify professional boundaries with @HelenOwen3 asking a very pertinent question on whether it was based around scope of practice or professionalism. Thus a subsequent question was asked ‘Where do we�?draw the line re: our boundaries in professional practice crossing boundaries with other health professioanls?�?Lots of answers flooded in around recognising our boundaries and enforcing our professions code of conduct in particular two tweets that highlighted the need was that off @joshpoole ‘scope of practice, representing your professional/ governing body, CPD‘ and @neil_maltby ‘knowing your limitations, skill set, and when to pass on‘ I found these two examples to be highly relevant to our scope of practice. If we consider the profession of physiotherapy we have a very multi-dimensional profession branching into many aspects of healthcare, the last time I checked physiotherapy had over 20 sub-professions branching from medical care to sports physiotherapy to alternative health, with additional scopes in nutrition, sleep hygiene, psychology etc.
A further sub-question was asked ‘Are we moving into an era, where overlap of boundaries is more important for the benefit of the healthcare system/patient/client?�?Lots of great answers came from this questions with a general consensus that it was helpful to patients to cross boundaries with @gwyn_owen highlighting�?‘2 me prof boundary=a moving line that defines the being/doing autonomous problem-solving in a particular discipline’ �?It highlighted that all clinicians �?participating in the physiotalk understood that it was beneficial to the patient to be able to deliver knowledge in other aspects of healthcare thus providing a holistic approach but at the same time recognising where our weaknesses lie and referring on appropriately. �?There was further consensus that this should be within the physiotherapy profession as well with @sophm14 tweeting ‘we must take responsibility and know whether we are out of scope if we question it then maybe shouldn’t’ .
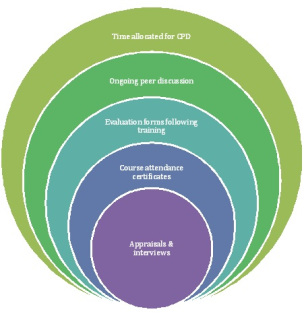
@prof_ieuanellis highlighted�?‘Prof boundaries historically established & linked to territorial defensiveness 2 resist change in roles & scope of practice’�?identifying that there were continuing issues with inter-disciplinary working. We all go through individual training to be the skilled clinician we strive for. At any one time patients may see several clinicians all offering their own opinion and thoughts�?regarding what is right and wrong for the patient. Crossing those boundaries can make a very controversial and confrontational environment for other clinicians and often be very confusing for patients. Sometimes we need to bite our tongue no matter how right or wrong we think the advice of another clinician may be, hence why the it is important to acknowledge inter-disciplinary working as opposed to multi-disciplinary team working. The two mean very different forms of team working. Question 1 concluded with an image highlighting the importance of lifelong learning when it came to understanding professional boundaries and scope of practice.
Moving onto�?Question 2:�?How is professional practice/boundaries valuable for the growth of our profession and other professions?�?and�?Question 3:�?How does the current plurality of our professional scope effect interprofessional relationships? I have placed these two questions together asthey tended to merge into each other.
@wigmore_welsh opened with a blinder�?‘Is the profession disintegrating and developing too many factions & fragmented sections with small boundaries?’�?highlighting that perhaps we have too many sub-divisions which is unhealthy for the profession itself. Further tweets came in to support the notion that perhaps we should get better at what we do best. @adammeakins ‘are we at risk of losing core values/skills if we diverge too much, shouldn’t we just focus on what we do best’�?and @northlightphys supporting this with�?‘ There is so much *depth* to work in to within our own�?professional- do core stuff to our best before diversifying’�?and @_joemiddleton offering�?‘I sometimes feel the prof has diverged too much too fast. We’re travelling faster than we can generate the research to justify!’�?
It was refreshing to see so many tweets acknowledging the importance of IDT working @pipwhitept tweeted�?‘do boundaries blur or just evolve? Think latter and this represents dynamism in prof’�?identifying a dynamic movement in professionalism and professional boundaries. This also highlighted that as evidence begins to shift more towards a connection between aspects of our lifestyles then so does healthcare need to evolve. @knowpainmike tweeted ‘Is it time for #CPD to embrace interprofessional learning? There are 6 different professions in this pic’�?

and @melrosestewart1 adding�?‘Ug nurses & physio students identify more similarities than diffs btwn their professions!’,�?@helenowen3 adding�?‘We all have the same core skills - wide and varied interests reflects population who we’re serving’�?and @adiemusfree pointing out similarities between physiotherapy and occupational therapy ‘ I think #chronicpain ed is encouraging interprofessionalism, not much difference btw you & me within therapy’.�?It appeared that a collaboration in disciplines ditching the ‘my way is the only way approach’ was something that we were all open too as clinicians. Finally @joshpoole tweeted�?‘its how we are being trained, interprofcollaboration for better future MDT working’ �?and @sportmednews�?expressed a strong opinion�?‘IMO having a clinical specialty + interprofessional learning is key. We need to know how to work as team, not free for all’. These comments highlighted a good understanding of the need for specialism but understanding that knowing when to refer and respecting�?other professional specialism was key to providing holistic care to patients.
Something I strongly agreed with was @wigmore_welsh highlighting an unsettling reality ‘How can we claw back practice we ‘abandoned’ such as #exercise have we lost the boundary 2B #exs professionals’�?This was the basis of my Crossfit write-up back in November and where this may cause a contradictory thought on my part I do believe that protecting our profession is an important aspect of our professionalism. �?Yet the more we move into interdisciplinary working there may be more blurring of our boundaries as @wigmore_welsh further pointed out�?‘will we move to a time we have a global profession the same boundaries? With #EU changes afoot I can see it happen’�?it appeared that some were happy to have a degree of blurring to provide better care. @viconeill26 tweeted ‘Blurring and improving knowledge is fine if done for the right reasons and not pushed on due to finances’ and�?@melrosestewart1 tweeted’ Blurred�?boundaries�?engenders criticality in CPD guided by codes of conduct’�?and @gwyn_owen tweeting�?‘do intra-prof boundaries allow us 2 trace how PT has responded 2 opps/time =>id/practice 2 multiply?’�?However blurring did bring some frustration but was this more down to individual professions not getting their message across about their role? @Bluffe94 pointed out quite rightly ‘many professionals think that we mobilise pts. Even when we do we are continuously analysing, assessing + planning further rx’�?which appeared to suggest that education of roles was not transparent amongst professionals. @helenowen3 responded ‘Agree! Saw CF patient on ward + nurse said didn’t need to as cud already walk - need to increase awareness of role’ @_joemiddleton added�?‘ Indeed! But do we tell enough people that that is what we are doing?’ with a further wagging finger comment ‘And if you do think all you’re doing is walking a pt or getting them out of bed…’
Furthermore an nice little conversation emerged between @jstjohnmatthews and�?@AndyMcdonough1:�?@jstjohnmatthews�?‘Is there a role for other #weAHPs in defining competency gold-standards if there is role-blurring?’�?�?‘P.S. Radiographer lurking in the background- but also AHP CPD Lead :-)’�?@AndyMcdonough1�?‘ definitely, work closely alongside ANP’s (nurses) and we share training and cpd.’�?@jstjohnmatthews ‘ employer sounds ace 🙂 #physiotalk. My MSc. project had a section on designing competencies so an interest’ @AndyMcdonough1�?‘in a new role so learning as we go a little but senior support, clinical and managerial essential�?‘ It was great to see clinicians sharing their experiences of IDT working and�?their successes in IDT application.
The chat ended on a high question 4 asked:�?How can we tackle issues around experiential bias?
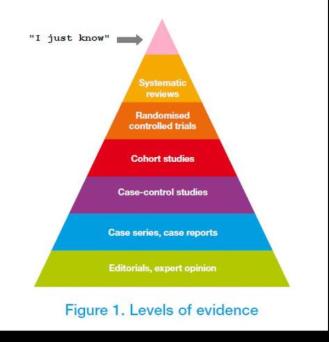
@physiotalk added a further question�?‘How often do we come across the ‘I just know’ - need to challenge?’ �?There were a whole host of comments one that stood out was @physiomorag ‘unfortunately far too often. Think that all too often ego gets in the way of EBP and CPD’ A lot of tweets flew in from students�?particularly around feeling unsettled during placements @sophm14 commented�?‘definitely, my last place I was confident to share, couldn’t say that about my first one though!’�?and @cuphysios asking�?‘I wonder how many students struggle to challenge their educator if they have a set way?’�?@helenowen3 frustrated commented ‘v. frustrating as a student to ask why and be told ‘because that’s just the way it’s done’.�?Unfortunately students seems to get a bad press because seniors don’t want to be seen as inexperienced and a hierarchical structure still dominates @hollykate94 tweeted ‘agreed, especially with the hierarchy can be hard to challenge senior views’�?and�?@uolphysio added�?‘ sometimes the fear of ‘don’t get on their bad side’ comes into effect. Fear of getting a lower grade’�?which is an unfortunate position for students as @_joemiddleton expressed ‘Sad to hear all the issues of experiential bias in practice and impact on students’.�?�?To be in such a position can affect their confidence as they are taught recent evidence and are encouraged to share as @sophm14 explained�?‘ students are taught up to date which we take to placement, if we are confident we can share’.�?Therefore highlighting the benefits of an integrated care approach with new knowledge from undergraduates. I want to add here that I am not chastising senior figures here it would appear to be beneficial to both parties if a reciprocal relationship of experience and new evidence helped to apply appropriate clinical reasoning @northlightphys made a valid point�?‘Experience is vital- but it started *somewhere* ie with some evidence. Evidence must inform/develop our experience’�?and further added�?‘Yup-Challenge culture! Ours were generous enough 2 realise we had more recent info’�?Again this further supports the need for all clinicians no matter what level of knowledge of experience to not be intimidated by seniority and to appreciate that we can all learn from each other.
Many other tweets came in around experiential bias around insecurity and defensiveness in clinicians that highlighted the possibility that some were not maintaining their practice in line with evidence base. It appeared that there was a gap increasing between the public and private model when it came to professional development issues such as training, supervision and courses, geared more towards benefiting the business rather than the identified developmental needs of the clinician. A lot more works needs to be done to stamp out experiential bias, hierarchy and dogma in all professions.
Too�?close I want to say thank you to everyone that participated in the chat it was my first acting as host and chair and I loved participants�?input and reaction! I apologise for not adding all the points as I think a few tweets didn’t make it onto the transcript as #physiotalk was not added. There were some awesome comments and a real insight into how we are all feeling regarding professional boundaries. It appears that most of us are more and more open to the idea of integrated care as we recognise the importance of inter-collaborative learning and the benefits towards holistic patient care.
Thanks again to everyone and thanks for having a read
TNP

Leave a Reply