

Whole of community pain health education. for back pain. Why does first-line care get almost no attention and what exactly are we waiting for?
I read with intrigue and interest Lorimer’s editorial in the British Journal of Sports Medicine (G. L. Moseley, 2018). I have huge respect for the man who has effectively flipped the traditionalist healthcare world upside down. Take physiotherapy for example, the scourge of biomedicalism and manual therapy is ingrained within all physiotherapists. Yet among them there are those that have shifted their practice to a more behavioural/activity approach (which could be imprudently misrepresented as a “hands off” approach) since much of the theoretical underpinnings of the postural, structural, biomechanical and manual therapy models have been refuted (Bereznick et al., 2002; Lederman, 2010, 2015; Schmidt et al., 2017; Van Ravesteijn et al., 2012).
I digress, back to Lorimer’s editorial. I have a big question. Undeniably Lorimer has devoted his life to understanding pain and for that I applaud him. Yet, within the first paragraph I became frustrated with his choice of words. I agree that the majority of back pain does not require surgery. I also agree that the majority of back pain does not require long term analgesics. I also agree that most will resolve over time. Yet the next part of that sentence stopped me in my tracks. ‘If we do not mess them up.’ I pondered on what he actually meant by that? If we assume he is talking about the patient there’s a really big BUT with that. If he meant the clinician there is also a big BUT with that! I want to return to both those points a little later but firstly focus on Lorimer’s main point – education. I won’t deny that education is incredibly important and that there is a significant amount of research that supports the use of education for pain management (Louw, Zimney, Puentedura, & Diener, 2016).
Yet there are many barriers to why pain education is not headline. Pain education’s integration within university curriculums (which is the corner stone of any healthcare training) is significantly lacking (Briggs, Carr, & Whittaker, 2011; Hoeger Bement & Sluka, 2015; Loeser & Schatman, 2017). Healthcare continues to be delivered under biomedicalism, educating clinicians with a language that represents pathology. This figuratively goes against the grain of pain education, and so changing that language with a proverbial click of the fingers is no easy feat. Lorimer himself identifies that clinicians do not have the understanding or resources to engage in what can be a complex and challenging exchange of health reconceptualization for the clinician and the recipient (L. Moseley, 2003) Yes, that paper is outdated but there are more recent publications that would support his paper (Domenech, Sánchez-Zuriaga, Segura-Ortí, Espejo-Tort, & Lisón, 2011; Gardner et al., 2017). My own experiences of working with other clinicians would appear to suggest that learning the complex neurobiology is fundamental prior to simplifying through the use of (say…) metaphor (the buzzword in healthcare) to facilitate reconceptualization.
That sentence…
So, let’s go back to the ‘if we do not mess them up’ comment and consider the reciprocal perspective between the patient and the clinician. There is much research that identifies the implications between clinician and recipient in communication, which is a skill in itself. Pain education is one small part of communication. Collaborative exchange of information without patrony is a challenge (Zanini, Sarzi-Puttini, Atzeni, Di Franco, & Rubinelli, 2015), as is clinician discomfort of risk of stigmatizing a patient (Synnott et al., 2015). The shift from medical, scientific terminology to understandable language has its challenges. Significantly, patients and clinicians define terms differently leading to misunderstandings when both think they are talking on common ground. Furthermore, recipients can choose and hear words important to them without considering the context of how the words are delivered (Barker, Reid, & Minns Lowe, 2009; Greville-Harris & Dieppe, 2015). Moreover, Patients seeking information from HCPs can experience difficulties understanding them and the medical literature (Darlow, 2016).
Now I am all for pain education, it is influential to my practice. However, i personally feel it is crucial that it is tied to activity. There is a wealth of evidence to support the importance of exercise/activity in the management of musculoskeletal pain (Babatunde et al., 2017; Brage, Ris, Falla, Søgaard, & Juul-Kristensen, 2015; Kroll, 2015; L. Moseley, 2002). However, there’s a but, again! Despite the extensive research in exercise dosage and health promotion, exercise/physical activity or health promotion is, like pain education, not a compulsory part of medical and physiotherapy training, with very little understanding of physical activity guidelines (Lowe, Littlewood, & McLean, 2018; Lowe, Littlewood, McLean, & Kilner, 2017; Weiler, Chew, Coombs, Hamer, & Stamatakis, 2012). So, the disciplines that have demonstrated a lack of uptake in pain education as identified in Lorimer’s editorial also demonstrate a lack of knowledge in exercise prescription. Tie that in with the universities not providing a basic grounding of exercise prescription or physiology, well, to me that is a crisis people!!
Jackasses and pain ed
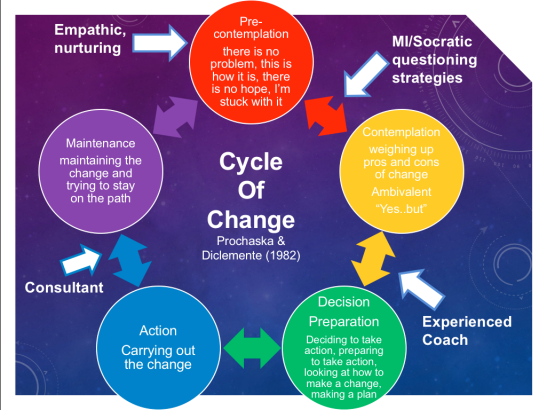
It is generally accepted that knowledge translation is important but essentially it is nothing more than that, the exchange of data between two individuals. I have previously stated pain education is one small part of an interchange between the individual living with pain and the clinician. It was Bill Fordyce that coined the phrase ‘Information is to behavior change as spaghetti is to a brick’. So, whilst explaining pain at front line care might help some people to get going again, for others we need to offer more. A further idiom that I would use to describe this issue – ‘A jackass can kick a barn down, but it takes a carpenter to build one.’ – Meaning that anyone can attempt to teach pain education but it takes more than just telling people that it is safe to move when they are avoidant of movement. As clinicians, we need to modify our role if we are to support people through the challenge of learning to live well with pain. Prochaska & Di Clemente, (1982) developed the trans-theoretical model of change. It suggests that our role should adapt as the person engages and goes through change – see image. So, whilst attempting to change the beliefs of patients through pain education it makes little difference if the person continues doing what they are doing. This is why (and this view is shared by many of my colleagues) I am probably a behaviourist.
I want to finish with a final thought. Should the title read ‘community pain education’ or should it read community health education, with the deletion of the words back pain?
Pain is a symptom of a larger emergent problem – poor health. When I say health, I don’t just mean the integration of bodily systems I mean health as a determinant of social integration and context. I have discussed the case for change in a previous blog.
Thanks for having a read.
TNP
References
Babatunde, O. O., Jordan, J. L., Van Der Windt, D. A., Hill, J. C., Foster, N. E., & Protheroe, J. (2017). Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence. PLoS ONE. https://doi.org/10.1371/journal.pone.0178621
Barker, K. L., Reid, M., & Minns Lowe, C. J. (2009). Divided by a lack of common language? A qualitative study exploring the use of language by health professionals treating back pain. BMC Musculoskeletal Disorders, 10, 123. https://doi.org/10.1186/1471-2474-10-123
Bereznick, D. E., Kim Ross, J., McGill, S. M., Kukkonen, J., Joukainen, a., Lehtinen, J., … Katz-leurer, M. (2002). The frictional properties at the thoracic skin-fascia interface: Implications in spine manipulation. Clinical Biomechanics, 17(4), 297–303. https://doi.org/10.1016/S0021-9290(02)00014-3
Brage, K., Ris, I., Falla, D., Søgaard, K., & Juul-Kristensen, B. (2015). Pain education combined with neck- and aerobic training is more effective at relieving chronic neck pain than pain education alone – A preliminary randomized controlled trial. Manual Therapy, 20(5), 686–693. https://doi.org/10.1016/j.math.2015.06.003
Briggs, E. V, Carr, E. C. J., & Whittaker, M. S. (2011). Survey of undergraduate pain curricula for healthcare professionals in the United Kingdom. European Journal of Pain (London, England), 15(8), 789–95. https://doi.org/10.1016/j.ejpain.2011.01.006
Darlow, B. (2016). Beliefs about back pain: The confluence of client, clinician and community. International Journal of Osteopathic Medicine. https://doi.org/10.1016/j.ijosm.2016.01.005
Domenech, J., Sánchez-Zuriaga, D., Segura-Ortí, E., Espejo-Tort, B., & Lisón, J. F. (2011). Impact of biomedical and biopsychosocial training sessions on the attitudes, beliefs, and recommendations of health care providers about low back pain: A randomised clinical trial. Pain, 152(11), 2557–2563. https://doi.org/10.1016/j.pain.2011.07.023
Gardner, T., Refshauge, K., Smith, L., McAuley, J., H?bscher, M., & Goodall, S. (2017). Physiotherapists? beliefs and attitudes influence clinical practice in chronic low back pain: a systematic review of quantitative and qualitative studies. Journal of Physiotherapy. https://doi.org/10.1016/j.jphys.2017.05.017
Greville-Harris, M., & Dieppe, P. (2015). Bad is more powerful than good: The nocebo response in medical consultations. American Journal of Medicine, 128(2), 126–129. https://doi.org/10.1016/j.amjmed.2014.08.031
Hoeger Bement, M. K., & Sluka, K. A. (2015). The current state of physical therapy pain curricula in the United States: A faculty survey. Journal of Pain, 16(2), 144–152. https://doi.org/10.1016/j.jpain.2014.11.001
Kroll, H. R. (2015). Exercise Therapy for Chronic Pain. Physical Medicine and Rehabilitation Clinics of North America, 26(2), 263–281. https://doi.org/10.1016/j.pmr.2014.12.007
Lederman, E. (2010). The fall of the postural–structural–biomechanical model in manual and physical therapies: Exemplified by lower back pain. CPDO Online Journal, 1–14.
Lederman, E. (2015). A process approach in manual and physical therapies: beyond the structural model.CPDO Online Journal, May, 1–18.
Loeser, J. D., & Schatman, M. E. (2017). Chronic pain management in medical education: a disastrous omission. Postgraduate Medicine, 129(3), 332–335. https://doi.org/10.1080/00325481.2017.1297668
Louw, A., Zimney, K., Puentedura, E. J., & Diener, I. (2016). The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiotherapy Theory and Practice, 3985(August), 1–24. https://doi.org/10.1080/09593985.2016.1194646
Lowe, A., Littlewood, C., & McLean, S. (2018). Understanding physical activity promotion in physiotherapy practice: A qualitative study. Musculoskeletal Science and Practice, 35(November 2017), 1–7. https://doi.org/10.1016/j.msksp.2018.01.009
Lowe, A., Littlewood, C., McLean, S., & Kilner, K. (2017). Physiotherapy and physical activity: a cross-sectional survey exploring physical activity promotion, knowledge of physical activity guidelines and the physical activity habits of UK physiotherapists. BMJ Open Sport & Exercise Medicine, 3(1), e000290. https://doi.org/10.1136/bmjsem-2017-000290
Moseley, G. L. (2018). Whole of community pain education for back pain. Why does first-line care get almost no attention and what exactly are we waiting for? British Journal of Sports Medicine, bjsports-2018-099567. https://doi.org/10.1136/bjsports-2018-099567
Moseley, L. (2002). Combined physiotherapy and education is efficacious for chronic low back pain. The Australian Journal of Physiotherapy, 48(4), 297–302. https://doi.org/10.1055/s-2004-813687
Moseley, L. (2003). Unraveling the barriers to reconceptualization of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. The Journal of Pain : Official Journal of the American Pain Society, 4(4), 184–9. https://doi.org/10.1016/S1526-5900(03)00488-7
Prochaska, J. O., & Di Clemente, C. C. (1982). Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy, 19(3), 276–288. https://doi.org/10.1037/h0088437
Schmidt, H., Bashkuev, M., Weerts, J., Graichen, F., Altenscheidt, J., Maier, C., & Reitmaier, S. (2017). How do we stand? Variations during repeated standing phases of asymptomatic subjects and low back pain patients. Journal of Biomechanics. https://doi.org/10.1016/j.jbiomech.2017.06.016
Synnott, A., O’Keeffe, M., Bunzli, S., Dankaerts, W., O’Sullivan, P., & O’Sullivan, K. (2015). Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: a systematic review. Journal of Physiotherapy, 61(2), 68–76. https://doi.org/10.1016/j.jphys.2015.02.016
Van Ravesteijn, H., Van Dijk, I., Darmon, D., Van de Laar, F., Lucassen, P., Olde Hartman, T., … Speckens, A. (2012). The reassuring value of diagnostic tests: A systematic review. Patient Education and Counseling, 86(1), 3–8. https://doi.org/10.1016/j.pec.2011.02.003
Weiler, R., Chew, S., Coombs, N., Hamer, M., & Stamatakis, E. (2012). Physical activity education in the undergraduate curricula of all UK medical schools: are tomorrow’s doctors equipped to follow clinical guidelines? British Journal of Sports Medicine, 46(14), 1024–1026. https://doi.org/10.1136/bjsports-2012-091380
Zanini, C., Sarzi-Puttini, P., Atzeni, F., Di Franco, M., & Rubinelli, S. (2015). Building bridges between doctors and patients: the design and pilot evaluation of a training session in argumentation for chronic pain experts. BMC Medical Education, 15(1), 89. https://doi.org/10.1186/s12909-015-0374-6

Leave a comment